 Search
Search
The following are the topics suggested for the first-trimester resident course:
–Indications for first-trimester ultrasound examination
–Gestational sac evaluation (intrauterine location, discriminatory human chorionic gonadotropin levels and differentiation from endometrial fluid)
–Yolk sac
–Amnion
–Embryo/fetus (number).
–Embryo/fetus cardiac activity; document with M-mode or movie clip
–Criteria for definitive diagnosis of embryonic/fetal death in the first trimester
–Components of sonographic dating in the first trimester
–Ultrasound evaluation of ampullary tubal ectopic pregnancy
–Subchorionic hematoma
–Sonographic features of molar pregnancy
–Association between thickened nuchal translucency and fetal chromosomal anomalies
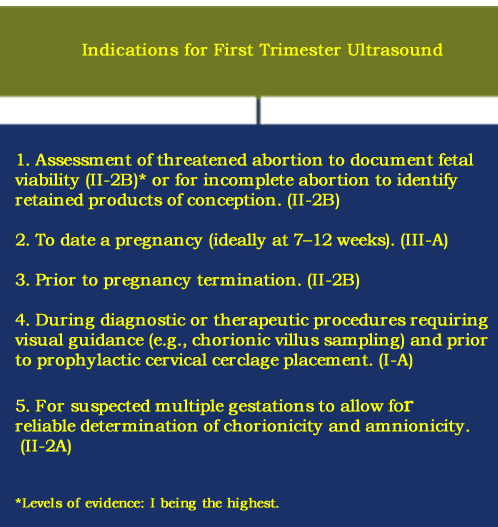
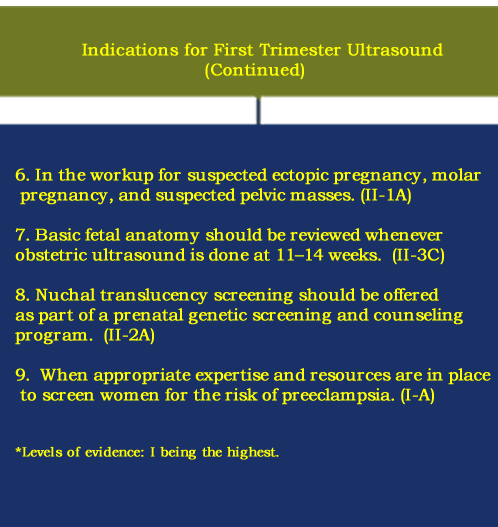
Indications for a First Trimester Ultrasound Examination
Preceded by pre-test counseling, women should be offered a first-trimester ultrasound (US) (11 to 13 6/7 weeks) according to ISUOG recommendations if there are clinical concerns, pathological symptoms, or specific indications. The full text of this article is available and provides details for the performance of the first-trimester fetal ultrasound scan. [1]
In 2019, the Society of Obstetricians and Gynecologists of Canada suggested the following recommendations for the performance of first-trimester ultrasound. https://www.jogc.com/article/S1701-2163(18)30762-X/fulltext
First Trimester Ultrasound Scan

Above left. Maternal ovary. Approximately 24 hours before ovulation, a hypoechoic ring within the GF is seen (cumulus oophorus), which contains the oocyte.
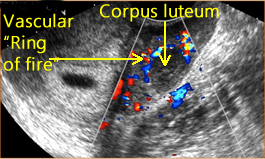
Above right. Maternal ovary. The corpus lutuem (CL) represents the ruptured GF, which is a thin-walled cyst with circumferential blood flow demonstrated by color Doppler. The CL secretes progesterone and a small amount of estrogen to stimulate endometrial proliferation.
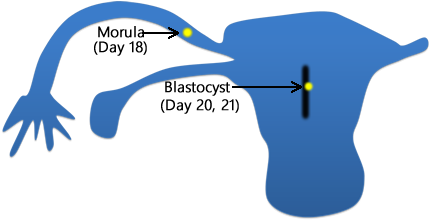
Above. After fertilization [2] the zygote undergoes rapid cell division and 3 days later, just before entering the uterus, the 12 to 16 cell stage (morula) is present. Within the uterus, the conceptus is termed the blastocyst.

Above. The blastocyst is composed of an outer cell layer, the trophoblast, which is destined to form part of the placenta and an inner cell layer, which is destined to form the embryo, amnion, umbilical cord, and yolk sac.
Chronology of Development
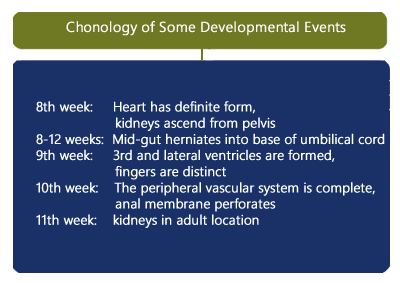
Above. The embryo undergoes some of the following developmental sequences. [3] By the 8th week, the heart has a definite form and by the 10th week, the peripheral vascular system is complete. By 8 to 12 weeks, the mid-gut herniates into the base of the umbilical cord. By the 9th week, the 3rd and lateral ventricles are formed, and the fingers are distinct. By the 10th week, the anal membrane perforates. The kidneys ascend from the pelvis in the 8th week and are in their adult location by the 11th week.
Gestational Sac Evaluation (Intrauterine Location)
Early Gestational Sac

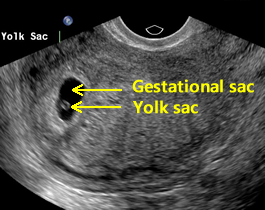
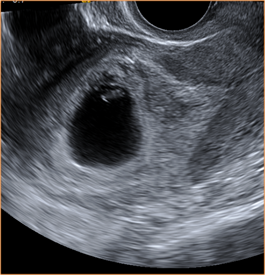
Above. The earliest sign of an intrauterine pregnancy (IUP) is a small gestational sac seen on transvaginal ultrasound at approximately 4 to 5 weeks and at that time, the mean sac diameter (MSD) is approximately 2.5 mm. The early sac should be round and adjacent to (not within) the linear interface of the endometrial lining, without displacing or deforming it.
This small round fluid collection (the chorionic cavity) is completely surrounded by a hyperechoic rim of tissue about 2 to 3 mm thick, which represents the developing chorionic villi and adjacent decidual tissue. The gestational sac is usually positioned in the mid to upper uterus.
Discriminatory hCG Levels
The discriminatory β-hCG level is the value above which an intrauterine gestational sac is seen on a consistent basis by ultrasound. This value is commonly cited as between 1000 and 2000 mIU per milliliter (World Health Organization 3rd or 4th International Standard). As noted by Doubilet and others, a single hCG level does not reliably distinguish among a normal intrauterine pregnancy, an ectopic pregnancy, or a nonviable pregnancy. [4] (Please see below).
Endometrial Fluid
During the first trimester, a small amount of fluid within the uterine cavity could be interpreted as a gestational sac. According to Radiopaedia.org, the findings of intrauterine fluid include: “generally irregularly-shaped (fluid) with pointed edges and/or filled with debris, sometimes referred to as ‘beaking’, centrally located in the endometrial cavity, rather than eccentrically located within the endometrium, displaces the anterior and posterior endometrial cavity surfaces, and does not demonstrate a yolk sac.”
Yolk Sac (YS)
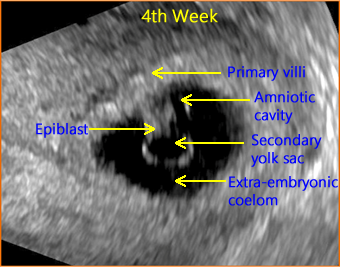
Above. The gestational sac is now visible and contains the secondary yolk sac lying opposite the amniotic cavity with the embryonic disk (epiblast) between them. The epiblast will go on to form the definitive embryo and fetus. The extra-embryonic coelom is the subsequent chorionic cavity (the space between the amnion and chorion). By about 14 weeks, the chorionic cavity is normally obliterated and the amnion-chorion membrane forms the amniotic sac within which is the amniotic fluid (“bag of waters”).
Decidua

Above. By 5 to 6 weeks, two concentric echogenic lines surround a portion of the gestational sac and can be seen on trans-abdominal ultrasound.
Above. On transvaginal ultrasound, note the decidua capsularis and the decidua parietalis, findings which are sometimes referred to as the double decidual sign. Note the YS which is typically the first structure visualized in an IUP on transvaginal ultrasound.
Gestational Sac

Above. On transvaginal ultrasound, a gestational sac is identified at 5 weeks. [5] In patients with accurate dates, cardiac motion is seen typically after 5 5/7 weeks, while a yolk sac is first seen at 5 1/7ths to 5 5/7ths weeks. [6] When an embryonic heartbeat is first seen, the MSD is 20 mm and at the time of embryo movements, the MSD reaches 30mm. [7]
The yolk sac has an echogenic periphery with a sonolucent center. Detection of a yolk sac confirms that the intrauterine fluid represents an IUP and the number of yolk sacs usually correspond to the number of amnions. Yolk sac number is useful in assessing amnion number in multiple gestations. The diameter of the yolk sac increases between 5 to 10 weeks to a maximum of about 6mm, [8] and the measurement of the yolk sac is usually from inner wall to inner wall.
Amnion and Chorion

Above. The origin of the chorion is different from that of the amnion since the outer cell layer of the blastocyst forms the chorionic membranes and the inner cell layer forms the amnion. The chorion and amnion usually fuse by about 14 weeks. Typically, the amnion is visualized after the YS.
Embryo/Fetus (Number)
At 6 to 8 weeks gestation, normal ranges are established for crown-rump length (CRL), heart rate (HR), gestational sac diameter (GSD), and yolk sac diameter (YSD). [9]
Above. Normal gestational sac with maximum YSD of 6.1 mm. Most recommend yolk sac measurement from the inner wall to inner wall as demonstrated.

Above. Normal gestational sac with yolk sac, amnion, and embryo at about 6 menstrual weeks. A complete survey is necessary of the gestational sac in both anterior-posterior and transverse views are necessary to count the number of embryos.

Above. Normal gestational sac and yolk sac at about 5 weeks.
Seen with transvaginal ultrasound (TVS) at about 5 weeks, the normal yolk sac (YS) is composed of 3 layers (ectodermal, mesodermal, and endodermal) and begins to regress after the 7th week, while the maximum diameter of the YS from 5 to 10 weeks is 5 mm to 6 mm. [10]
At 6 to 10 weeks, a deformed or absent yolk sac is not encountered in a normal pregnancy with a detected heartbeat. [11]
Normally, there is the sequential appearance of the yolk sac, HR, and amniotic membrane (amnion). The largest yolk sac in a continuing pregnancy is about 8.1 mm. In a first trimester pregnancy, the HR and YSD progressively increase. [12]
An intrauterine pregnancy (IUP) is typically diagnosed if there is a yolk sac, or a gestational sac with or without a fetal pole or a fetal pole with or without a HR.
Embryo/Fetus Cardiac Activity Documented with M-mode
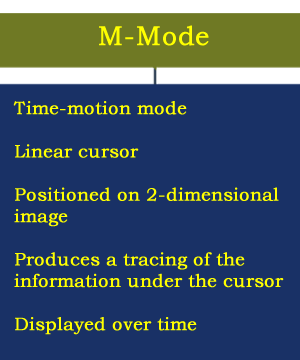
Activated as part of ultrasound instrumentation, M-Mode allows visualization of cardiac activity during the first-trimester exam. The characteristics of this methodology are listed in the above chart.
The above chart illustrates the information derived from an M-mode display. This information includes the fetal heart rate and the presence or absence of fetal cardiac activity.
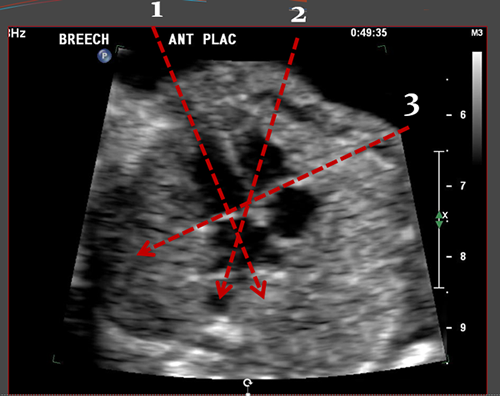
Subcostal or apical four-chamber views are the best methods to place the cusor to obtain M-mode data.
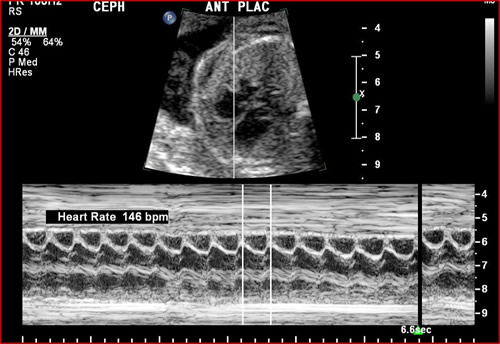
The above image demonstrates a typical M-mode image. A fetal heart rate of 146 beats per minute is confirmed.
Mean Sac Diameter (MSD)
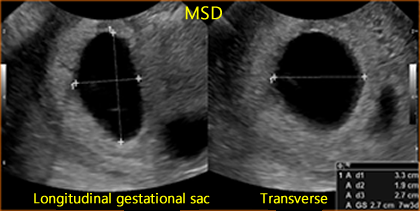
Above. The mean sac diameter (MSD) is usually 5 mm at by approximately 5 weeks. The MSD is calculated by adding 3 orthogonal dimensions of the chorionic cavity, excluding the hyper-echoic rim of tissue, and dividing by 3 (Length + Width + Height/3). MSD growth in normal gestation increases approximately 1.1 mm/day, while the embryo grows at 1 mm/day. [13]
Mid-gut Herniation
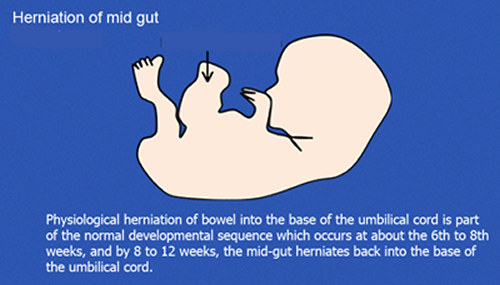
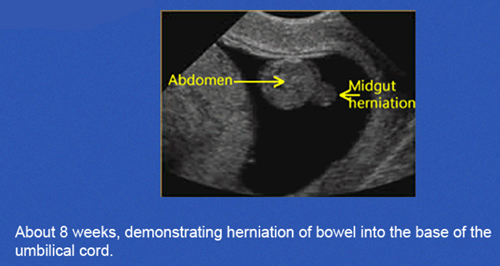
Above. Physiological herniation of bowel into the base of the umbilical cord is part of the normal developmental sequence which occurs at about the 6th to 8th weeks, and by 8 to 12 weeks, the mid-gut herniates back into the base of the umbilical cord.
Criteria for Definitive Diagnosis of Embryonic/Fetal Death in First Trimester
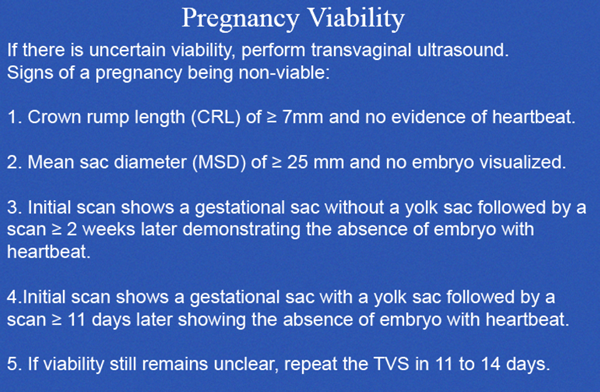
A recent review [14] defines pregnancy failure and specifies cutoff values for this purpose. Transvaginal ultrasound diagnosis of pregnancy failure in a pregnancy with uncertain viability is as follows:
CRL of ≥ 7 mm and no evidence of heartbeat.
MSD of ≥ 25 mm and no embryo visualized.
Initial scan shows a gestational sac without a yolk sac followed by a scan ≥ 2 weeks later demonstrating the absence of embryo with heartbeat.
Initial scan shows a gestational sac with a yolk sac followed by a scan ≥ 11 days later showing the absence of embryo with heartbeat.
If viability remains unclear, repeat transvaginal ultrasound in 11 to 14 days.
Patients with threatened abortion may exhibit a normal YSD or abnormal YSD. 40% of patients with missed abortions will have an abnormal YSD outside of the 5th to 95th confidence interval. [15]
Significant differences exist in YSD between normal pregnancies and those with spontaneous miscarriage and threatened abortions at < 12 weeks. [16]
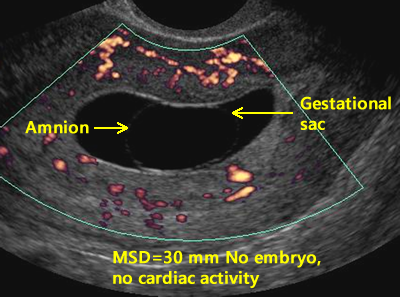
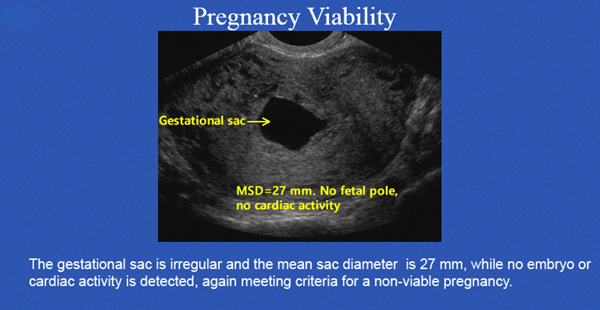
Above. In this case, no yolk sac is present and the MSD is ≥ 25 mm, while no embryo or cardiac activity is detected, meeting criteria for a non-viable pregnancy.
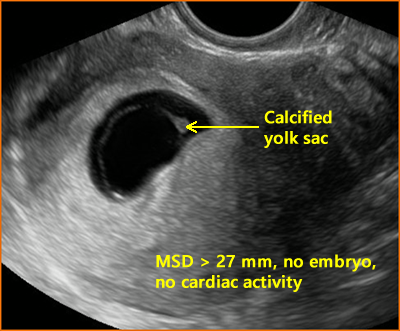
Above. In this case, the yolk sac (YS) is calcified and the MSD is ≥ 25 mm, while no embryo or cardiac activity is detected, again meeting criteria for a non-viable pregnancy.
In an embryonic gestation, the YS may be absent, irregular in shape, or relatively large. In a missed abortion with a prior HR, the YS may be relatively large, regressing, or deformed. [17]
In summary, the YS may be small, calcified, echogenic, irregularly shaped, or persistent in pregnancies destined for poor outcome, as noted in a sonographic pictorial of the YS. [18]
Termination of pregnancy should not be based on YS characteristics alone since a normal pregnancy may be ended. In a stable patient, follow-up ultrasound in 11 days to 2 weeks should be considered if other criteria for a non-viable pregnancy are not met.

Above. The gestational sac is irregular and meets criteria for a non-viable pregnancy.
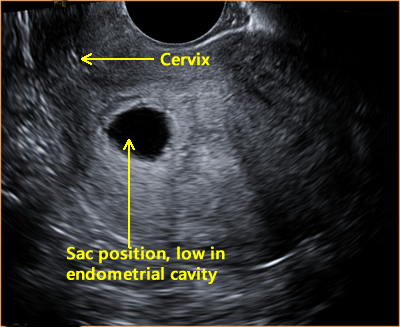
Above. While the sac position is low in the endometrial cavity, not all criteria are met for a non-viable pregnancy.
In a retrospective review, Hu, Poder, and Filly determined that only 12% of 1013 threatened abortions met these present conservative guidelines for non-viability as recommended by the Society of Radiologists. [19] Clearly, there is much room for improvement.
An important task is to define normality in the first trimester by correctly assigning whether a pregnancy is viable, nonviable, or in an ectopic location. The false positive rate (the incorrect diagnosis of a nonviable pregnancy when the pregnancy is normal) can be as high as 4.4%. [20]
Summary Pregnancy Viability


Components of Sonographic Dating in The First Trimester
The American College of Obstetricians and Gynecologists (ACOG) (Committee Opinion 611, October 2014) along with the American Institute of Ultrasound in Medicine, and the Society for Maternal-Fetal Medicine have issued recommendations for estimating gestational age and due date.
In summary:
1. The most accurate method to establish or confirm gestational age is a CRL taken up to 13 6/7 weeks.
2. In the case of assisted reproduction, the age of the embryo and the date of transfer should be used.
3. The last menstrual period (LMP), and the first accurate ultrasound examination should be the basis for the expected due date (EDD), discussed with the patient and recorded in the medical record.
4. Using criteria in the document, the best obstetric estimate is recommended for the purposes of clinical care while the criteria for research and surveillance are presented.
The following chart summarizes the guidelines for “Re-dating the pregnancy on the basis of the ultrasound findings” when there is a difference between the ultrasound dates and the LMP (last menstrual period).
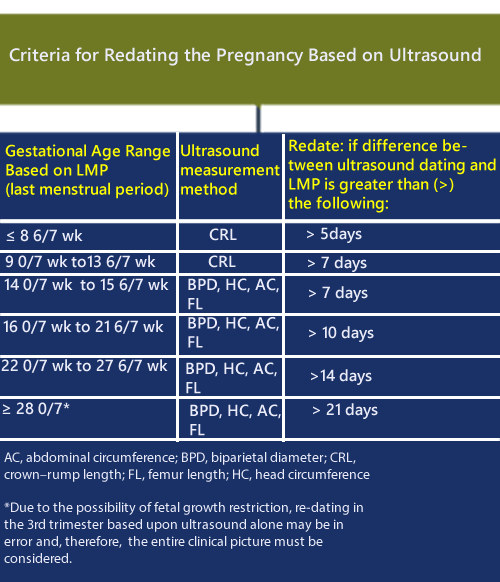
An update on methods for estimating due date is available here: Full Article (Updated 2017)
Due Date Calculator
A pregnancy due date and gestational age calculator is available here: http://perinatology.com/calculators/Due-Date.htm
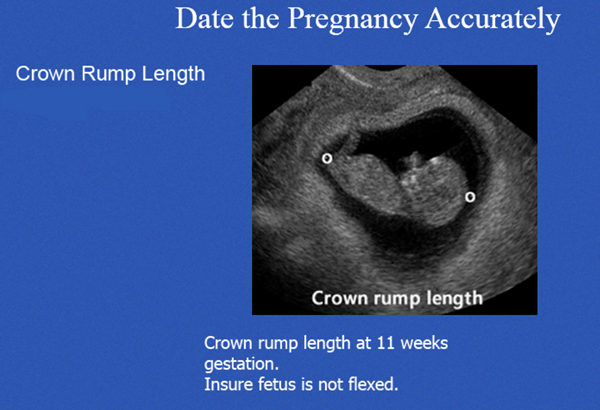
Crown Rump Length (CRL)
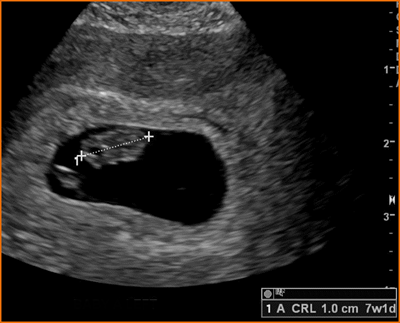
Above. Measured between 6 and 10 weeks, the CRL is the most accurate method for dating pregnancies. The longest axis of the embryo is measured and the yolk sac is identified separately from the embryo and is not included in the measurement.


Above. Fetal crown-rump length (CRL) as a function of gestational age (GA). Gray open circles: raw data. Black open circles: empirical means.


Normal CRL, 12 weeks 1 day
Charts are available from the open-access article “International standards for early fetal size and pregnancy dating based on ultrasound measurement of crown-rump length in the first trimester of pregnancy.” [21] (This article is freely downloadable). The purpose of the article is to establish international standards for CRL in relationship to gestational age.
A calculator is available on: Perinatology.com. If the CRL is known, the estimated gestational age and expected nuchal translucency can be obtained. If the NT measurement is known, the calculator will yield the NT percentile.
Ultrasound Evaluation of Ampullary Tubal Ectopic Pregnancy (EP)
.

Above. Location of tubal and non-tubal ectopic pregnancies. Most EPs occur in the ampulla or isthmus of the FT.
The classic triad for ectopic pregnancies is a pregnancy presenting with pain, bleeding, and the presence of a mass. Risk factors, which are reproductive failures, include history of tubal disease and smoking, which may help to establish a diagnostic and management strategy. [22] Other risk factors include, uterine anomalies, history of assisted reproduction, and pelvic infection.
On transvaginal ultrasound (TVS), a tubal ectopic pregnancy may be present if no intrauterine pregnancy (IUP) is seen. A definitive gestational sac with a yolk sac excludes the diagnosis, but fluid within the endometrial cavity in the absence of a YS does not exclude the diagnosis. Rarely, a heterotopic gestation may be present with one gestational sac consistent with an IUP and another simultaneous pregnancy which is ectopic in location. To confirm the likelihood of an tubal EP, one of the following conditions should be met [23]:
1. An inhomogeneous adnexal mass separate from the ovary.
2. An empty extra-uterine gestational sac with a hyperechoic ring in the adnexal region.
3. An extrauterine sac in the adnexal region with a yolk sac or fetal pole ± cardiac activity.

Above. Tubal ectopic pregnancy. Note empty gestational sac surrounded by increased vascularity in the adnexa region.

Above. Tubal ectopic pregnancy. Note inhomogeneous mass surrounded by increased vascularity in the left adnexa.
A pregnancy diagnosis is sometimes made but the location of the pregnancy is not readily apparent. In 2011, a consensus statement of definitions and outcomes for pregnancy of unknown location (PUL) was published. [24]
The following categories for ultrasound diagnosis were suggested:
1. Definite EP: Extrauterine gestational sac with yolk sac and/or embryo (with or without cardiac activity).
2. Probable EP: Inhomogeneous adnexal mass or extrauterine sac-like structure.
3. PUL: No signs of either EP or IUP.
4. Probable IUP: Intrauterine echogenic sac-like structure.
5. Definite IUP: Intrauterine gestational sac with yolk sac and/or embryo (with or without cardiac activity).
Treatment for tubal EP is either medical with methotrexate, or surgical by laparoscopy. Many protocols suggest periodic hCG measurements and transvaginal ultrasound.
Some treatment protocols recommend medical management in patients with suspected ectopic pregnancy if the β-hCG level is <1 000 IU/l, the patient is asymptomatic, and the EP is not visualized. However, a single β-hCG level cannot exclude the possibility of an intrauterine pregnancy, and despite numerous studies and meta-analysis, no single protocol or method of management has been established. At least 6 diagnostic protocols have been defined using a combination of ultrasound, β-hCG, and serum progesterone. [25] Finally, serum β-hCG may not be useful in distinguishing IUPs from ETs in symptomatic pregnant women. [26]
The following observations relate to treatment and recurrence risk [27]:
1. Irrespective of treatment mode, the chances of a subsequent successful IUP in EP patients are the same.
2. Generally, the size of the EP should not be a limiting factor for conservative laparoscopic surgery.
3. The risk of recurrent EP is about 10% after salpingectomy.
Ectopic Pregnancy: Non-Tubal
Ectopic pregnancies, which occur in locations other than the fallopian tube, are characterized by delayed diagnosis and increased morbidity compared with tubal EPs. These pregnancies include interstitial pregnancy (implantation in the interstitial portion of the FT), cornual pregnancy (rudimentary horn of unicornuate uterus), cervical pregnancy (and caesarean scar pregnancy), and ovarian pregnancy.
Subchorionic Hematoma
About 20% of all pregnancies are associated with bleeding and pain during the first trimester, while most of these pregnancies will progress uneventfully. [28]
Bleeding may be due to threatened, incomplete, or spontaneous abortion; ectopic pregnancy or gestational trophoblastic disease. Genetic abnormalities account for 50% to 70% of spontaneous abortions, while 20% of patients with first trimester bleeding have a subchorionic bleed or hematoma. [29]
Another 10% to 15% of patients with first trimester bleeding will have an ectopic pregnancy. [30]
Spontaneous abortion
Spontaneous abortion is defined as the loss of a pregnancy prior to the completion of 24 weeks gestation. The main maternal symptoms are bleeding and pain. If a fetal HR has been detected, the risk of spontaneous abortion in singletons is 12.2%. [31]
In twin gestations, a significant CRL discrepancy at 7 weeks to 9 6/7 weeks is associated with the loss of one twin, while a discrepancy of <2 0% is associated with a 97% rate of viable twin pregnancies. [32]
Incomplete Spontaneous Abortion

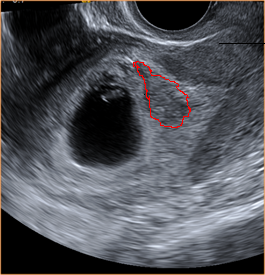
Above. Incomplete spontaneous abortion with “products of conception” (POC), which can include trophoblastic tissue, clot, and embryonic remnants.
Incomplete spontaneous abortion occurs when there is partial passage of POC. Retained products remain within the endometrial cavity and the risk for continued maternal bleeding remains. TVS in the sagittal, transverse, and oblique planes can be used to assess the uterine contents. The presence of heterogeneous, irregular tissue with or without the presence of a gestational sac distorts the endometrial mid-line echo. [33]
Examples of First Trimester Bleeding
First trimester bleeding may be mild and insignificant or profuse. Resolution of subchorionic bleeding and clot is possible and observation of bleeding over time can change from acute, to chronic, to resolved.
Above. Note area of outlined bleeding, which is acute.

Above. Note area of chronic bleeding about 1 week after acute episode. Fetal cardiac activity and fetal growth are normal.

Above. Same patient, 2 weeks later. Image demonstrates resolution of subchorionic bleeding.

Above. 11 6/7 weeks gestation. Note the anterior placenta and the amnion chorion separation from the chorionic plate. The anechoic area represents fluid and or blood.


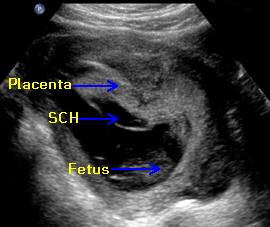
Above. First trimester SCH (subchorionic bleed). The relative positions of the amnion and chorion are illustrated. There is an extensive anechoic collection of fluid and blood in the subchorionic space.


Above. At the margin of the placenta, the amnion chorion membrane is elevated. The mixed echoes suggest clot between the amnion and chorion while there is fluid or blood in the subchorionic space and some evidence of marginal acute bleeding.


Above. Extensive hematoma in a woman with chronic bleeding. This represents a mixed pattern with anechoic areas suggesting fluid or blood and the mixed echos suggesting clot formation.


Above. Again, extensive hematoma in a woman with chronic bleeding. This represents a mixed pattern with anechoic areas suggesting fluid or blood and the mixed echos suggesting clot formation. In addition, the small echogenic particles representing blood fragments within the amniotic fluid are consistent with a history of maternal bleeding.
Blood clots may be present and are avascular and irregular on color Doppler. After confirmation of incomplete abortion on TVS, the patient may choose surgical evacuation or expectant management. Expectant management with close medical follow-up may be successful. In one study, 83% of women who chose expectant management spontaneously completed the process by week 2. [34]
Complete Spontaneous Abortion
A complete spontaneous abortion occurs when the endometrial cavity is empty of the products of conception after a prior diagnosis of an IUP was established. A pregnancy of unknown location (PUL) occurs when there is no evidence for an IUP or ectopic pregnancy on TVS. A failing pregnancy can be suspected but not confirmed if the serum β-hCG declines 13% or more over a 48 hour period. [35]
On TVS, no evidence for products of conception are noted within the endometrial cavity in complete spontaneous abortion. Scan planes are the same as those established for incomplete spontaneous abortion.
Sonographic Features of Molar Pregnancy
Gestational trophoblastic neoplasia (GTN) terminology includes complete hydatidiform mole (CHM), partial hydatidiform mole (PHM), invasive mole, choriocarcinoma, and placental site trophoblastic tumor. These neoplastic changes in placental trophoblastic tissue are typically associated with increased hCG production and may have other clinical manifestations such as early onset preeclampsia, hyperemesis, and bleeding. Among the GTN subtypes, HM is the most common occurring at a frequency of 1 in 750 pregnancies. [36]
In CHM, there is generalized trophoblastic hyperplasia and swelling of the chorionic villi in the absence of an embryo or fetus, while in PHM, there is focal trophoblastic hyperplasia and focal swelling of villous tissue in the presence of fetal or embryonic tissue. [37]
Complete moles are paternally derived and partial moles are usually triploid.


Above. Placental triploidy. Note multiple clusters of grape-like cysts. The ultrasound appearance is “snow storm,” but this finding is less likely in the first trimester. (Images on triploidy are courtesy of Jane JK Burns, AS, RDMS).
There has been an evolution in the presentation of HM since the widespread introduction of obstetrical ultrasound. With routine first trimester ultrasound, 41% of the patients with CHM are asymptomatic. [38] Most HM pregnancies are evacuated during the first trimester and both the ultrasound features and the histopathology of the specimens are different compared to mid-trimester late diagnosis of HM. A majority of histologically proven HM are associated with a sonographic diagnosis of missed abortion or anembryonic pregnancy. [39]

Above. Note first trimester molar changes.
First trimester molar pregnancies may demonstrate cystic changes or increased placental echos with a diagnosis of CHM more likely at ≥ 13 weeks, but only 50% of the cases were diagnosed before 13 weeks. [40] Molar pregnancies have been diagnosed in 88% of CHM [41], and in a review of 16 patients, only 9 (56%) demonstrated the classic “snow storm” appearance. [42]
In a retrospective review of 1053 cases of partial or complete HM, a pre-evacuation diagnosis was made in 44% of cases with a final diagnosis of HM. Partial moles were detected less often compared with complete moles. [43]
Jauniaux and Nicolaides reported that 10 of 11 patients with either CHM or PHM demonstrated sonographic placental changes at 10 to 14 weeks, which included diffuse cystic lesions and multicystic ovaries in all patients with a β-hCG of > 8 MoM. [44] As suggested by these authors, cytogenetic investigation should be offered, while Β-hCG measurements and Doppler ultrasound measurements of the uterine artery may improve diagnostic potential. Routine histological examination of the products of conception is warranted as well as a follow-up regimen for the detection of persistent trophoblastic neoplasia.
Association Between Thickened Nuchal Translucency (NT) and Fetal Chromosomal Anomalies






Above: 12 weeks 1 day. Normal Mid-line NT

Above: 12 weeks 1 day. Normal Mid-line NT. Note the amnion which is below the area of amnion measurement.
Above. Normal NT.
Above. Increased NT.
The NT (See Genetic Markers) measures posterior neck nuchal fluid and a measurement of > 3 mm is always abnormal and is a marker for fetal aneuploidy and certain malformations, especially the heart.
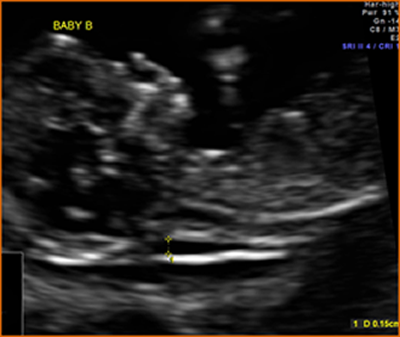
The NT is measured at a gestation age of 11w0d to 13w6d weeks with a corresponding CRL of between 45 mm and 84 mm. A mid-sagittal view is taken in a neutral position away from the amnion. The maximum translucency is obtained with the callipers “on-to-on” as illustrated. A certification program is available through: The Fetal Medicine Foundation.
NT and Adverse Pregnancy Outcomes

In addition to its strong association with fetal aneuploidies, increased NT is linked to the risk of adverse perinatal outcomes including fetal malformations, dysplasia, deformations, disruptions, and genetic syndromes, but these risks do not reach significance until the NT is ≥ 3.5 mm (> 99th percentile). [45] The fetal death rate depends upon the degree of abnormality of the NT (at 3.5-4.4 mm, death rate = 2.7%, at >6.5 mm, death rate = 19%). [46] Alternatively, if the fetus survives to the mid-trimester and no abnormalities are noted on the targeted scan, the risk of adverse outcome does not significantly increase. [47]
Specialized training and certification for sonographers is required for the NT measurement. A certification program is available through The Fetal Medicine Foundation.
A calculator is available on Perinatology.com. If the CRL is known, the estimated gestational age and expected nuchal translucency can be obtained. If the NT measurement is known, the calculator will yield the NT percentile.
code]15200773[/notecode]
Normal Images
Normal First Trimester Images
Measurements
Anatomy can be defined and some standard fetal measurements can be taken during the first trimester.

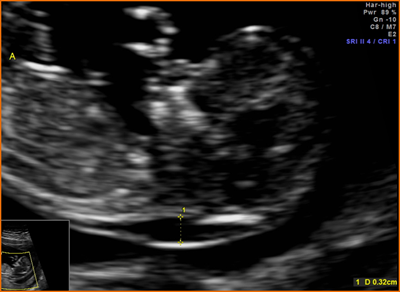
Above. BPD (biparietal diameter) and HC (head circumference) taken at 13 3/7 weeks.
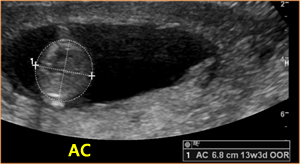
Above. AC (abdominal circumference) taken at 13 3/7 weeks.

Above. FL (femur length) taken at 13 3/7 weeks.
Criteria for definitive diagnosis of embryonic/fetal death in the first trimester.


Above. Crown rump length, 11 weeks.


Above. The rhombencephalon is normally visualized between 7 and 9 weeks.


Above. Note embryonic rhombencephalon and fetal extremities.


Above. Axial view. Fetal skull and brain, 12 weeks


Above. Sagittal view, 11 weeks. Note upper and lower extremities.


Above. Fetal hand, 13 weeks.


Above. Fetal lower extremities, 13 weeks.


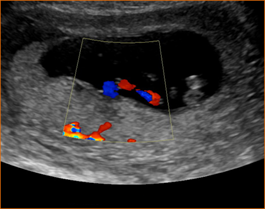
Above. 4 chamber cardiac view, 13 weeks. Caution: Color Doppler in the first trimester should be used only when the benefit exceeds the risk.


Above. Stomach and umbilical cord, 13 weeks.


Above. Umbilical arteries and bladder, 13 weeks.

Above. Umbilical cord placental insertion, 13 weeks.
Acknowledgments: A number of images are courtesy of Jill Beithon RT, RDMS, RDCS, RVT
References
After completing the course, to take the quiz: Click Here.
[‘wp_objects_pdf’]
-
Abstract: PMID: 23280739 Moore, KL, Persaud TVN, Shiota, K. In Color Atlas of Clinical Embryology. WB Saunders Company; 1994; p.1. Rumack, CM, Wilson SR, Charboneau, JW. In: Diagnostic ultrasound. Mosby, St. Louis, 1998, p 977. -
Abstract: PMID: 24106937 -
Abstract: PMID: 2030862 -
Abstract: PMID: 2660539 -
Abstract: PMID: 2030862 Rumack, CM, Wilson SR, Charboneau, JW. In: Diagnostic ultrasound. Mosby, St. Louis, 1998, p 997. -
Abstract: PMID: 20847544 -
Abstract: PMID: 22215774 -
Abstract: PMID: 16953856 -
Abstract: PMID: 17693010 Rumack, CM, Wilson SR, Charboneau, JW. In: Diagnostic ultrasound. Mosby, St. Louis, 1998, p 990. -
Abstract: PMID: 24106937 -
Abstract: PMID: 9435738 -
Abstract: PMID: 24779249 -
Abstract: PMID: 16953856 -
Abstract: PMID: 22215774 -
Abstract: PMID: 25154939 -
Abstract: PMID: 21997898 -
Abstract: PMID: 25044000 -
Abstract: PMID: 15388673 -
Abstract: PMID: 17468257 -
Abstract: PMID: 20947073 -
Abstract: PMID: 15388673 -
Abstract: PMID: 21310509 -
Abstract: PMID: 15388673 -
Abstract: PMID: 24841987 -
Abstract: PMID: 15905817 -
Abstract: PMID: 24841987 -
Abstract: PMID: 12871890 -
Abstract: PMID: 19521968 -
Abstract: PMID: 12099260 -
Abstract: PMID: 12099260 -
Abstract: PMID: 17468257 -
Abstract: PMID: 2414703 -
Abstract: PMID: 9060124 -
Abstract: PMID: 10985617 -
Abstract: PMID: 15846756 -
Abstract: PMID: 10478967 -
Abstract: PMID: 10985617 -
Abstract: PMID: 10478967 -
Abstract: PMID: 16273594 -
Abstract: PMID: 9060124 -
Abstract: PMID: 15846173 -
Abstract: PMID: 23814750 -
Abstract: PMID: 15846173
2
3
8
13