 Search
Search
Normal CNS Critical Anatomy and Normal Ultrasound of the Fetal Brain
(To view a reference. Click on the reference number which will take you to the abstract or article.)

Schematic of the human brain showing connections between the cerebrum and the midbrain. The relationship between the lateral ventricle, thalamus, and cerebellum are demonstrated. These are all key fetal sonographic relationships. Above figure. [1]

Human brain, frontal (coronal) section. The divisions of the brain are seen here in a frontal (coronal) slice of the brain: 1. Cerebrum, 2. Thalamus, 3. Mesencephalon – Midbrain, 4. Pons, 5. Medulla oblongata, 6. Medulla spinalis – Spinal cord. Above figure. [2]
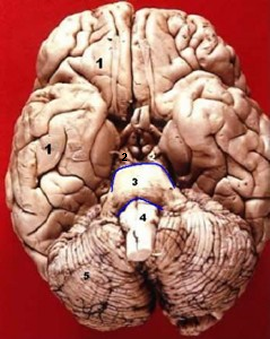
1. Cerebrum
2. Mesencephalon – Midbrain
3. Pons
4. Medulla oblongata
5. Cerebellum
Above figure. [3]

Sagittal section through the brain showing the cerebellum and the corpus callosum. Above figure. [4]

Sagittal section through the brain showing greater detail including the 3rd and 4th ventricle and the septum pellucidum. Above figure. [5]

Vertebral column demonstrating the 7 cervical vertebrae, the 12 thoracic vertebrae, and the 5 lumbar vertebrae. Above figure. [6]
The last rib is attached to the 12th thoracic vertebra (T-12), a useful landmark in the fetus.

This is a transverse view of the spine showing the vertebral body, spinous process, lamina, and articular process. Above figure. [7]
Normal CNS Embryology and Early Development

Above. The developing embryo is demonstrated at approximately Day 11. The arrow points to the epiblast or the embryonic disc, the cells of which are destined to form the fetus. A primitive streak develops from the epiblast by day 17 and by day 19, a notochordal* process occurs, with primitive neural folds by about day 23. By day 25, the first somites appear and by day 28, the neural folds begin to fuse. [8]
*from the mesoderm of the 3 cell layers which include ectoderm and endoderm.

Above:
A. The precursor of the neural crest is ectoderm which is induced by a primary neural induction process most likely originating from the notochord and occurring from approximately day 19 to day 23. [9]
B. At around day 23, the neural folds begin to appear and fuse by day 29.
C. The neural tube is destined to form the brain and the spinal cord.
D. The continued folding of the ectoderm and endoderm fuse to form the body cavity.
Above figure. [10]

Above. The development of the central nervous system undergoes a process of neurulation.
Primary neurulation: the folding of the neural folds to form the neural tube.
Secondary neurulation: the neural development in the caudal (lower) part of the embryo by an indifferent cell mass known as the caudal eminence or end-bud. The region of secondary neurulation is induced by the caudal eminence.

Above. In the 4th week, the upper part of the neural tube bends at the level of the future midbrain (the Mesencephalon). The Prosencephalon is the future fore-brain, and below the mid-brain is the hind-brain, the Rhombencephalon.
Above figure. [11]

Above. The prosencephalon consists of the telencephalon which forms the cerebral hemispheres, and the diencephalon which forms the optic and thalamic tissues.
The mesencephalon mid-brain remains unchanged and forms a portion of the brain stem (tectum, cerebral peduncle, pretectum, and mesencephalic duct). The rhombencephalon consists of the metencephalon and myelencephalon.
The metencephalon forms the part of the brain stem which includes the pons and cerebellum, and the myelencephalon forms the part of the brain stem which includes the medulla oblongata. Above figure. [12]

Above. The relative anatomic locations of the forebrain, midbrain, and hindbrain in the human fetus.
Normal CNS Later Development

The formation is demonstrated of central nervous system anatomic areas as derived from the forebrain (prosencephalon), the midbrain (mesencephalon), and the hindbrain (rhombencephalon). The forebrain and hindbrain form 2 divisions while the midbrain remains as one. [13]
Nerve Development

A two-step process is involved in neuron development. Neurons differentiate from stem cell precursors, migrate, and develop axons, which is an activity-independent mechanism guided by genetic programs within the neuron. The activity-dependent mechanism takes place once the neurons reach their target area. These processes are complex and involve numerous mediators. [14]
Neurons travel from their site of origin to their final place within the brain by radial, tangential, or multipolar migration.

The development of the critical central nerve pathways is present at the 6-week embryological stage.
Above figure: [2]
1. olfactory, 2. optic, 3. oculomotor, 4. trochlear, 5. trigeminal sensory, 6. trigeminal motor, 7. abducens, 8. facial, 9. vestibulocochlear, 10. glossopharyngeal, 11. vagus, 12. cranial accessory, 13. spinal accessory, 14. hypoglossal, 15. cervical I, II, III, and IV.

The spinal cord is composed of a dorsal (top) sensory portion. Ectoderm induces the development of the roof plate with BMP (Bone Morphogenetic Proteins). The ventral (bottom) or motor floor plate is induced by the notochord or mesoderm layer. Above figure. [15] The sensory nerves are primarily afferent in function ( go towards the cord) while the motor nerves are primarily efferent (go away from the cord). [16]. These nerves are functional and fetal movement has been observed as early as 5.5 weeks post-fertilization. [17]

Day 20: A demonstration the developing somites, the precursor of which is the mesoderm which is lateral to the neural tube (paraxial). Above figure. [18]
The somites give rise to the: [19]
1. dermatome
2. myotome
3. sclerotome
Somite formation begins about the 3rd week post-fertilization. A total of 52 somites are formed. In the human, the first four somites form the basi-occipital bone of the skull while the next 33 somites form the vertebrae. Above figure. [4]
The remaining somites then degenerate.
A complex process of somite formation occurs which includes: notch signaling, boundary formation, epithelialization, and axis specification. These processes require multiple gene specifications, proteins, and other substances. Above figure. [4]
Summary

This is a summary of major embryological events in the formation of the human central nervous system. Note that the distal tip of the cord is different during fetal life compared to the adult distal tip of the spinal cord. [20]
Normal CNS Ultrasound Brain Anatomy
Normal CNS Video
Above. Normal fetal CNS at 22 2/7ths weeks. Video courtesy of Dr. Mayank Chowdhury; Pallav Imaging Institute, Mayflower Women’s Hospital, Ahmedabad, India.
Above. Key fetal anatomy includes the choroid plexus, the septum cavum pellucidi (SCP), the lateral ventricles, and the corpus callosum. The pericallosal artery is a continuation of the anterior cerebral artery and it continues superiorly and posteriorly supplying the corpus callosum and the medial aspect of the cerebral hemisphere.
Key Views
There are three major scan planes for the fetal brain which accommodate 3 views:
1. Thalamic view
2. Ventricular view
3. Cerebellar view
The thalamic view is taken at the level of the biparietal diameter (BPD) and head circumference (HC).
The ventricular view is obtained through the atrium of the lateral ventricle.
The cerebellar view is angled through the posterior fossa (cisterna magna). All are axial (transverse) views of the fetal head with the exception of the cerebellar view, which is axial oblique. Other planes include the sagittal, parasagittal, and coronal which may be useful or necessary to define anatomy.
Thalamic View


Above. Thalamic view at 20 weeks. Note the thalamus and the position of the ambient cistern. The fornices are noted which are distinguished from the cavum septi pellucidi (CSP) by 3 parallel lines instead of the box-like structure of the CSP.


Above. Thalamic view at 33 weeks gestation. Note the 3rd ventricle and again the fornices.

Above. This is the same acquisition plane for the BPD and HC. Visualization of the thalami, the midline falx, and the box-like cavum septi pellucidi (CSP) are possible. The presence or absence of the CSP is key to defining abnormal brain anatomy.
Ventricular View



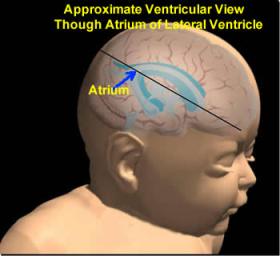
Above. This is a schematic of the lateral ventricles demonstrating the frontal, occipital, and temporal horns with the atrium of the lateral ventricle at the confluence of the occipital horn. The axial plane will demonstrate the lateral ventricles and the choroid plexus.


Above. This is an axial view demonstrating the atria of the lateral ventricle and the choroid plexus. The measurement is within normal limits.
Cerebellar View




Above. The cerebellar view is axial oblique with rotation of the transducer from the thalamic view to the cerebellum, while obtaining a view of the central cerebellar echogenic vermis. This view allows visualization of the cerebellum and cisterna magna (posterior fossa).
Cerebellar Measurements


Above. The cisterna magna or posterior fossa measurement is taken as illustrated from the outer aspect of the cerebellar vermis to the internal side of the occipital bone, and is normally between 2 mm and 10 mm in depth. The transcerebellar diameter is also measured as illustrated from outer to outer aspect of the cerebellum and varies by gestational age. Note the box-like cavum septi pellucidi (CSP) which can also be seen with the cerebellar view.
Sagittal View
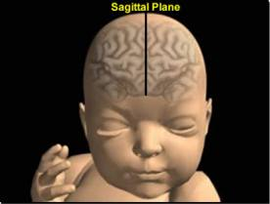

Above. The approximate sagittal plane will demonstrate the corpus callosum, cavum septi pellucidi, and cavum vergae as well as the nasal bone.
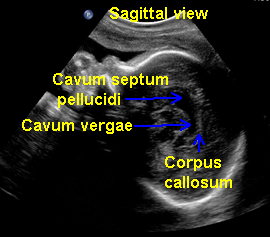

Above. The sagittal midline view of the brain. Note the corpus callosum, cavum septi pellucidi, and cavum vergae.
Parasagittal View
Above. Approximate parasagittal view. The parasagittal view allows visualization of the atrium, body, and anterior horn of the lateral ventricle and of the choroid plexus. It is not a commonly used view, but may be helpful in visualizing the atrium and the choroid plexus when the fetus is in breech presentation and the axial view is difficult to obtain.


Coronal View


Above. The approximate coronal views which can demonstrate the lateral ventricles, especially the frontal horns in an effort to determine whether there is fusion across the midline. The midbrain, choroid plexus, and cerebellum can also be assessed in this plane.




Above. This coronal view demonstrates the body of lateral ventricles and the midbrain. The coronal view may also demonstrate the echogenic choroid plexus. This view may be more easily obtained when the fetus is in breech presentation.
The transverse axial view permits visualization and measurement of the lateral ventricles as well as critical head measurements. It affords a view of the contents within the ventricle (blood or tumors) as well as an assessment of intracranial calcifications. The midsagittal view of the fetal brain best accomplishes visualization of the corpus callosum, cavum septum pellucidum, and posterior fossa.

Above. In breech presentation and transverse lie of the fetus, the midsagittal view can be obtained with a transabdominal scanning plane. With cephalic presentation, a transvaginal approach gives the best opportunity for midsagittal visualization. [21] The visualization of the septum pellucidum in all instances is helpful. Coronal views are useful for defining the site of ventricular communication and confirming the absence of the corpus callosum.

Above. Prenatal ultrasound evaluation of the fetal brain requires observation of specific structures, which in turn verify normality of other CNS structures. [22]

Above. The cavum septum pellucidum (CSP) and the cisterna magna (CM) are visible on trans-abdominal ultrasound between 16 weeks and 38 weeks. [2] Specific measurements of the CSP and CM differ significantly between the second and third trimester and correlate with biparietal diameter and gestational age. [23]

Above. The cavum septi pellucidi is critical to the diagnosis of a number of CNS malformations. [24] The presence of the CSP excludes complete agenesis of the corpus callosum while the absence of the CSP suggests the possibility of a number of other intracranial abnormalities, including septo-optic dysplasia.

Above. Septo-optic dysplasia is associated with a number of intracranial abnormalities. [25]

To define associated CNS malformations, other imaging modalities or views are necessary in addition to those obtained by routine trans-abdominal axial scan. These methods include transvaginal 2-D ultrasound and 3-D ultrasound. Above. 2-D transabdominal and transvaginal ultrasound may be the initial imaging modality of choice for schizencephaly, followed by 3-D ultrasound and fetal MRI. [26]
References
Figure: This is a file from the National Institute of Health, Resources, Graphics Gallery. Source: Neuroscience: http://www.niaaa.nih.gov/Resources/GraphicsGallery/Neuroscience/Pages/211p67.aspx. Figure: This is a file from the Wikimedia Commons. Date: 30 November 2005. Source: http://www.healcentral.org/healapp/showMetadata?metadataId=40566. Author: John A Beal, PhD. Department of Cellular Biology & Anatomy, Louisiana State University Health Sciences Center Shreveport. Permission (Reusing this file) CC-BY. Figure: This is a file from the Wikimedia Commons. Date: 30 November 2005. Source: http://www.healcentral.org/healapp/showMetadata?metadataId=40566. Author: John A Beal, PhD. Department of Cellular Biology & Anatomy, Louisiana State University Health Sciences Center Shreveport. Permission (Reusing this file) CC-BY. Figure: This is a file from the Wikimedia Commons. Source: http://upload.wikimedia.org/wikipedia/commons/6/6b/Illu_pituit. Figure: This is a file from the Wikimedia Commons. Originally from Gray’s Anatomy. Copyright expired. Source: http://upload.wikimedia.org/wikipedia/commons/3/36/Gray768. Figure: This is a file from the Wikimedia Commons. Source: http://en.wikipedia.org/wiki/File:Gray_111_-_Vertebral_column-coloured.png. This image (or other media file) is in the public domain because its copyright has expired. Figure: This is a file from the Wikimedia Commons. (Modified). Source: http://en.wikipedia.org/wiki/File:Corpusvertebrae.png. This image (or other media file) is in the public domain because its copyright has expired. O’Rahilly, R. and Muller F., Human Embryology and Teratology. Second Edition. Wiley-Liss. 1996. pages 361-401. O’Rahilly, R. and Muller F., Human Embryology and Teratology. Second Edition. Wiley-Liss. 1996. pages 361-401. Source: http://en.wikipedia.org/wiki/Neural_crest Source: http://en.wikipedia.org/wiki/Neural_development_in_humans
Figure: http://en.wikipedia.org/wiki/File:4_week_embryo_brain.jpg. Copyright released into the public domain.Figure: http://en.wikipedia.org/wiki/File:EmbryonicBrain.svg. This is a file from the Wikimedia Commons. Permission is granted to copy, distribute, and/or modify this document under the terms of the GNU Free Documentation License, Version 1.2 or any later version published by the Free Software Foundation. O’Rahilly, R and Muller F. Human Embryology and Teratology. Second Edition. Wiley-Liss. 1996. pages 361-401. http://en.wikipedia.org/wiki/Neural_development_in_humans. Figure: http://en.wikipedia.org/wiki/File:6_week_human_embryo_nervous_system.svg. This is a file from the Wikimedia Commons. Date: May 4, 2010. Source: Own work. Author. Kurzon. Copyright of work released into the public domain.
Figure: http://en.wikipedia.org/wiki/File:Spinal_cord_direv.svg. This is a file from the Wikimedia Commons. This file is licensed under the Creative Commons Attribution-Share Alike 2.5 Generic license. O’Rahilly, R and Muller F. Human Embryology and Teratology. Second Edition. Wiley-Liss. 1996. pages 361-401. O’Rahilly, R and Muller F. Human Embryology and Teratology. Second Edition. Wiley-Liss. 1996. pages 361-401. http://en.wikipedia.org/wiki/Somite. Figure: http://en.wikipedia.org/wiki/File:Gray20.png. This is a file from the Wikimedia Commons. This image is in the public domain because its copyright has expired. This applies worldwide.
O’Rahilly, R and Muller F. Human Embryology and Teratology. Second Edition. Wiley-Liss. 1996. pages 361-401. O’Rahilly, R and Muller F. Human Embryology and Teratology. Second Edition. Wiley-Liss. 1996. pages 361-401. -
Abstract: PMID: 16238537 -
Abstract: PMID: 16344747 -
Abstract: PMID: 12692827 -
Abstract: PMID: 20194938 Septo-optic dysplasia. Erin E, Leonhardt BS, Tan-Sinn P. Journal of Diagnostic Medical Sonography. 2005; 21(6): 479-486. -
Abstract: PMID: 19536862
1
2
3
4
5
6
{kind=link}
7
{kind=link}
8
9
10
11
{kind=link}
12
{kind=link}
13
14
{kind=link}
15
{kind=link}
16
17
18
{kind=link}
19
20
25