 Search
Search
Abruptio Placenta
Vasa Previa
Chorioangioma
Abruptio Placenta
Page Links: Definition, Incidence, Etiology, Risk Factors, Recurrence Risk, Clinical Associations, Outcome, Summary, References
Definition
Abruptio placenta is the separation of the normally implanted placenta from the myometrium or uterine wall.
There are two main subcategories:
• Concealed: maternal hemorrhage not visible.
• External or not concealed maternal hemorrhage.
Other useful categories include the timing of clinical events by trimester of pregnancy and their associated ultrasound findings.


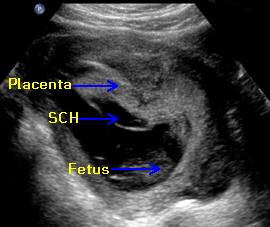
Above left. This schematic of a retroplacental hemorrhage demonstrates total detachment of the placenta.
Above right. Partial detachment of the placenta is present with extension of hemorrhage to the subchorionic space.
Abruptio placenta presents clinically as a spectrum of events, and the ultrasound findings are varied. First trimester symptoms include bleeding and ultrasound findings of subchorionic bleeding, while second or third trimester hemorrhage may present in a clinical sequence that makes assessment by ultrasound more difficult depending upon the location, extent, and duration of the bleeding.
Incidence
The incidence of abruptio placenta is approximately 1% to 2% of all pregnancies [1],[2], while placental abruption complicates 5.1% of preterm deliveries. [3] The rates of abruption in African American women have increased from 0.76% to 1.43%, a 92% increase during 2 comparable time periods, while the rate in Caucasian women increased by 15%. [4]
Etiology
The etiology of abruptio placenta is unknown. Possibilities include:
• The failure of fetal membranes to normally form at about 9 weeks’ gestation results in subchorionic bleeding.[5]
• Early pregnancy changes link severe growth restriction and abruption. [6]
• Chronic histologic changes in the placenta, umbilical cord, and membranes may be associated with abruptio placenta. [7]
• Humoral immune response of the mother to the fetus is suggested by IL-6 increase, which is observed in patients with abruption. [8]
• Thrombophilia (Factor V Leiden may influence the course of placental abruption). [9]

Finally, in patients needing immediate delivery for abruptio placenta, both Leiden factor V and Factor II A20210 are elevated. [10]
Risk Factors

Above left. Maternal risk factors associated with placental abruption are listed and include prior abruptio, smoking, trauma, drug use, premature rupture of the membranes (PROM), and advanced maternal age (AMA). [2]
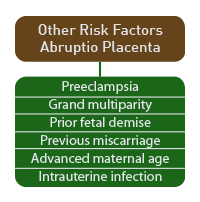
Above right. In a population with an incidence of abruption of 0.57%, other risk factors are possible. The relative risk (RR) vary from 4.39 for preeclampsia to 1.55 for previous miscarriage. Most cases of placental abruptio occur before labor in low-risk populations and are not predictable. [11]
Recurrence Risks

The greatest recurrence risk is a history of previous abruption (11.9% versus a background risk of 0.7%). [12]
Clinical Associations
Other risk factors include bleeding, hypertension, and growth restriction, while placental type and maternal biomarkers may be associated risk factors.

Above. Overall clinical associations with abruptio placenta are illustrated.
Bleeding
An episode of bleeding at < 20 weeks increases the relative risk for abruption to 1.6 compared to women without bleeding. [13] The risk of abruption is 3.58 times higher among women with premature rupture of membranes (PROM) compared to women without PROM. [14]
Hypertension and fetal growth restriction
Chronic hypertension increases the rate of abruption from 15.6 per 1000 pregnancies compared to 5.8 per 1000 pregnancies in women who are not hypertensive. [15]
Pregnancies complicated by severe growth restriction are more likely to be associated with abruption, particularly those at less than the first percentile weight. These women are 9 times as likely to have a birth associated with abruption compared to those with weights of > 90th percentile. [16] Infants with low birth weight are more common in patients with abruption. This association with premature delivery occurs in both growth restricted and appropriate for gestational age infants. [17]
Placental type
Circumvallate and circummarginate placenta are associated with placental abruption. [18] In women with circumvallate placenta, the odds ratio for placental abruption is increased to 13.1 (95% confidence limits: 5.65 to 30.2). [19]
Potential Maternal Biomarkers
C-Reactive protein and chlamydial antibody levels in early pregnancy do not predict placental abruption. [20] Further, antiangiogenic levels of sEng are elevated before the onset of hypertension and placental abruption. [20] sEng, PGF (placental growth factor) and sFLT-1 levels during the early trimester do not predict abruptio placenta. [21],[22]
Other
C-section with first live birth also increases the risk of abruption with a subsequent pregnancy. [23]
Outcome
• The perinatal mortality is high (119/1000) in abruptio placenta compared to controls (8.2/1000). [16]
• Mortality is also higher at every gestational age, and 55% of excess deaths are due to premature delivery. [16]
• Fetal death is common in cases of abruption when more than 50% of the placenta is detached. [2]
• Most cases of abruption occur before labor and are not always predictable. [11]

Because of variations in clinical presentation, both maternal clinical course and ultrasound findings are important in defining outcome. First trimester presentations may be different from mid-trimester or third trimester presentations. For example, first trimester symptoms of vaginal bleeding are different from an acute later-term event due to trauma or maternal drug abuse such as cocaine.
The incidence of an intrauterine hematoma is 3.1% during the first trimester in a general obstetric population. [24] While there is debate as to the clinical significance of subchorionic and retroplacental hematomas detected during the first trimester, the reported frequency is as high as 18% between gestational ages 9 to 25 weeks [25],[26],[27],[28]. Most studies support adverse events in women with ultrasound defined retroplacental or subchorionic hemorrhage.
Fetal Outcome
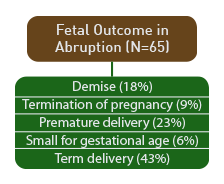

Above left. Fetal outcome in 65 surviving patients with placental abruption and placental hemorrhage is as follows: fetal demise in 18%, (TOP) termination of pregnancy in 9%, premature delivery in 23%, fetal growth restriction in 6%, and term delivery in 43%.[29]
Above right. Important outcome variables include the amount, location, and size of the hemorrhage. [29]

Above. In 516 patients with vaginal bleeding, large hematomas had almost twice the rate of loss compared with small and moderate sized hematomas. [30]

Above. In the Faster consortium trials of 16,506 patients, bleeding at 8 weeks’ or less was a risk factor for spontaneous loss prior to 24 weeks’ gestation. [31]

Above. Similarly, in the Faster trial, maternal age of greater than 35 was a risk factor for spontaneous loss prior to 24 weeks. [31] In the same study, heavy bleeding during the first trimester is a risk factor for premature delivery and placental abruption. [31] In a series of 21 patients, poor prognosis was noted for SCH with a 71% unfavorable outcome.
Clinical factors important for prognosis include: relative and absolute size of the hematoma, presence of pain, severity of vaginal bleeding, and change in hematoma size at follow-up visits. No correlation was noted between outcome and echogenicity of hematoma, presence of marginal elevation, gestational age, maternal age, parity, or gravidity. [32]
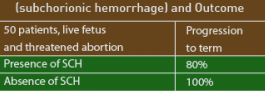
Above. In 50 patients with a live fetus at 9 weeks’ gestation or greater with a history of threatened abortion, those demonstrating the presence of SCH on ultrasound had a poorer prognosis compared to those with the absence of SCH on ultrasound. [33]
Summary
Definition:
Abruptio placenta is the separation of the normally implanted placenta from the myometrium or uterine wall.
Incidence:
• 1% to 2% of all pregnancies. [1],[2]
• 5.1% of preterm deliveries. [3]

Etiology:
Multifaceted:
• Failure of fetal membranes to form normally at about 9 weeks. [5]
• Severe growth restriction and abruption. [6]
• Chronic histologic changes in the placenta, umbilical cord, and membranes. [7]
• Humoral immune response of the mother to the fetus suggested by IL-6 increase in patients with abruption. [8]
• Thrombophilia (Factor II and Factor V Leiden may influence the course of placental abruption). [9]
Important clinical associations are:
• Bleeding at 20 weeks relative risk 1.6. [7]
• Premature rupture of membranes (PROM): RR = 3.58. [14]
• Chronic hypertension: 15.6/1000 pregnancies versus 5.8/1000 non-hypertensive pregnancies. [15]
• Severe growth restriction: 9 times as likely versus fetal weights > 90th percentile. [16]
• Circumvallate and circummarginate placenta: odds ratio increased 13.1. [19]

In the presence of maternal bleeding, placenta previa should be excluded. Transvaginal ultrasound can be useful early in gestation to define the extent of the hemorrhage. The amount, location, and size of the hemorrhage are important variables in defining outcome as well as maternal symptoms of pain.

If the bleeding is greater than 2.0 cm from the internal cervical os (ICO) at 19 weeks’ or less, look for findings associated with subchorionic hemorrhage, such as the presence of subchorionic fluid. At greater than 20 weeks’ gestation in the presence of maternal bleeding, retroplacental or intra-placental clot may not be seen. In both cases, clinical factors are important, such as duration, size, and location of the hemorrhage.
First trimester or early mid-trimester changes [34],[35] include:
• Extrachorionic and complex collections of fluid or blood.
• Crescent-shaped collections of fluid or blood.
• Absence of echoes in the subchorionic space.
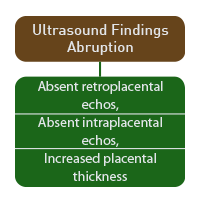
Second trimester or third trimester ultrasound findings [36] include:
• Wide range of echogenicity depending upon timing.
• Acute bleeding that may be difficult to distinguish from placental tissue.
• Increased placental thickness.
• Rounded or separated placental edges.


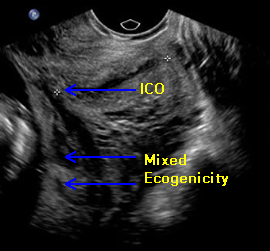
Above left. First trimester subchorionic bleed with anechoic collection of fluid and blood in the subchorionic space.
Above right. Mid-trimester, a pattern of mixed placental echogenicity with portions of subchorionic space are anechoic, while other portions demonstrate a mixed echogenic pattern. In the Faster consortium of 16,506 patients, heavy bleeding during the first trimester was a risk factor for premature delivery and placental abruption. [31]
Abruptio Placenta: Imaging Considerations

The findings on ultrasound depend on the time at which the bleeding occurs in relation to the performance of the ultrasound. Acute hemorrhage is hypoechoic or isoechoic compared to the placenta, while chronic hemorrhage may demonstrate sonolucent areas. [37]
A subchorionic hemorrhage is more likely to be recognized at less than 20 weeks gestation. [1]

Most hematomas are subchorionic, while retroplacental hematomas account for less than 20% of the total and pre-placental hematomas account for less than 5%. [1]

Above left. The ultrasound findings in abruptio placenta should also be viewed according to gestational age and maternal symptoms. Performed in the second or third trimesters, ultrasound findings are likely to be diverse and include a wide range of echogenicity depending on timing. Acute bleeding is sometimes difficult to distinguish from placental tissue and it becomes necessary to seek other ultrasound findings such as placental thickness, and the character of the edges. [1],[38],[39],[40]
Above right. Subchorionic hemorrhage noted in the first trimester is more likely to contain extra-chorionic concentrations of fluid which may be crescent-shaped. [41],[42],[43]
Abruptio Placenta: Images
Subchorionic Bleeding and Abruptio Placenta

Above. 11 6/7 weeks gestation. Note the anterior placenta and the amnion chorion separation from the chorionic plate. The anechoic area represents fluid and/or blood.


Above. First trimester SCH (subchorionic bleed). The relative positions of the amnion and chorion are illustrated. There is an extensive anechoic collection of fluid and blood in the subchorionic space.


Above. At the margin of the placenta, the amnion chorion membrane is elevated. The mixed echoes suggest clot between the amnion and chorion while there is fluid or blood in the subchorionic space and some evidence of marginal acute bleeding.


Above. Extensive hematoma in a woman with chronic bleeding. This represents a mixed pattern with anechoic areas suggesting fluid or blood and the mixed echos suggesting clot formation.


Above. Again, extensive hematoma in a woman with chronic bleeding. This represents a mixed pattern with anechoic areas suggesting fluid or blood and the mixed echos suggesting clot formation. In addition, the small echogenic particles representing blood fragments within the amniotic fluid are consistent with a history of maternal bleeding.


Above. Mid-trimester scan in a patient with chronic bleeding. This likely represents a marginal placental abruption with the clots demonstrating differences in age. Note the hyper-echogenic area compared to the clot near the placental margin.


Above. Chronic abruptio placenta. Note placental texture compared to the clot with a mixed echogenic pattern near the ICO (internal cervical os).

Above. Mid-trimester scan in a patient with low-lying posterior placenta and chronic bleeding. Note the pattern of mixed echogenicity and the extension to the internal cervical os (ICO) area is primarily clot from the chronic abruptio placenta.
Abruptio Placenta: Video
Above. Patient 1. Large subchorionic hematoma in a woman with chronic bleeding during the mid-trimester. Mixed echogenic pattern suggests blood clot, while anechoic areas suggest blood or fluid. The amnion/chorion membrane is fused and freely mobile.
Above. Patient 1 (continued). Large subchorionic hematoma during the mid-trimester. Mixed echogenic pattern suggests blood clot, while anechoic areas suggest blood or fluid. Note mobile organized clot.
Above. Patient 2. Note placenta is located on the anterior uterine wall. At the margin of the placenta are mixed echoes suggestive of hemorrhage and clot formation. On the posterior uterine wall, there is amnion/chorion separation suggestive of subchorionic hemorrhage.
Above. Patient 2 (continued). This view illustrates the amnion/chorion separation and the anechoic pattern consistent with fluid or blood.
Go to top
Vasa Previa: Information
Page Links: Definition, Etiology, Incidence, Risk Factors, Diagnosis, Ultrasound Accuracy and Vasa Previa, 3-D in Diagnosis of Vasa Previa, Mortality, Prevention/Treatment, References
Definition
Vasa previa is defined as the presence of fetal blood vessels at or near the internal cervical os. These vessels are exposed to spontaneous rupture or compression and rupture at the time of amniotomy or labor. The total fetal blood volume is relatively small and blood loss from vessel rupture can result in exsanguination and death.


Above. Color Doppler image of vasa previa. The cervix is demonstrated and the region of the ICO (internal cervical os). The vessels are seen traversing this area and are confirmed to be fetal in origin by Doppler velocimetry.
Etiology

Etiology of Vasa Previa:
A. Velamentous insertions near the internal cervical os: The cord inserts into membranes and exposed vessels cross the internal cervical os (Occurrence: 25% to 62%). [44]
B. Exposed vessels cross the internal cervical os between a separate extra lobe of the placenta (succenturiate or bilobed) and the main placental mass (occurrence: 33% to 75%). [1]
C. Second trimester placenta previa: Involution of a portion of placenta previa leaves vessels exposed over the internal cervical os. (Occurrence up to 69%). [45]
Incidence
• 1 in 2000 to 1 in 5000 births [46],[47],[48]
• Recent retrospective series (1 in 1310 births ) [49]
Risk Factors
Risk Factors / Odds Ratio (OR)
• IVF Pregnancy [50] / 7.75 (OR)
• Bilobed or succenturiate placenta [6] / 22.11 (OR)
• Second trimester placenta previa [6] / 22.86 (OR)
• Velamentous cord insertion
• Cord insertion into lower 1/3 of uterus (occurs 11% of time but it’s occurrence is associated with placental malformation and accessory placenta) [51],[52]
• Late pregnancy bleeding [53]
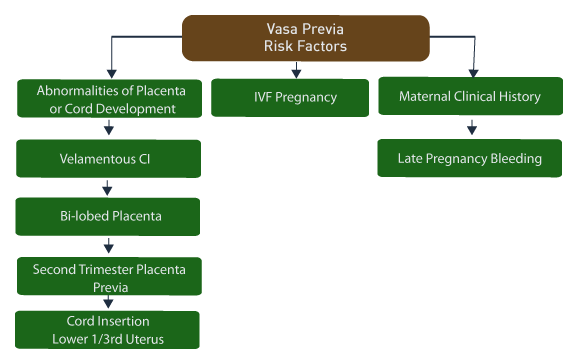
Above. A summary of risk factors is presented.
Diagnosis
Assess carefully the following group of patients, those with:
• Gray scale echogenic parallel or circular lines (umbilical cord) near the internal cervical os. [54]
• Velamentous cord insertion particularly if low cord insertion site. [7]
• Extra lobe of the placenta, especially if in the lower 1/3 of the uterus. [7]
• History of second trimester placenta previa. [6]
• Low cord insertion site. [7]
If any of the above findings are present, perform color Doppler transvaginal ultrasound of the internal cervical os region [10]
Ultrasound Accuracy and Vasa Previa
A recent systematic review of the accuracy of ultrasound in the diagnosis of vasa previa included 583 articles of which two were prospective and six were retrospective cohort studies. [55] Whether transvaginal ultrasound (TVS) is used for primary evaluation or for evaluation after vasa previa is suspected on transabdominal scan, TVS with color Doppler is the superior method for evaluation. Transvaginal color Doppler in the second trimester resulted in 100% sensitivity and 99.0% to 99.8% sensitivity.
3-D in Diagnosis of Vasa Previa
3-D ultrasound may complement the diagnosis:
Look for multiplanar and surface rendered views of fetal vessels over the internal cervical os. [56],[57],[58]
Assess 3-D axial view of endocervical canal and visualize fetal vessels in relationship to internal cervical os. [11]
Mortality/Morbidity

In undetected cases of vasa previa, fetal mortality has been reported as high as 30% to 100% due to rupture of fetal vessels and fetal blood loss. [2]
Mortality depends upon antenatal diagnosis. [59] Recent data, cited above, suggests survival is as high as 97% if the diagnosis is made antenatally while the survival is lower if the diagnosis is not made. [15]
Prevention/Treatment
Prevention of fetal death:
• Prenatal diagnosis by ultrasound is essential. C-section delivery should be performed before the onset of fetal membrane rupture with the potential for fetal umbilical vessel rupture. Recommended gestational age for preventive C-section is not uniform, but some authors suggest 35 weeks gestation in the absence of ruptured membranes or labor. [15]
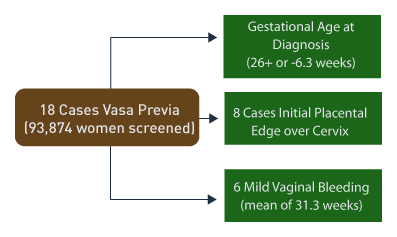
Lee, et al [11] studied 18 cases of vasa previa screened by ultrasound with overall excellent outcomes. In that report, there were 2 deaths, one fetal and one neonatal.
Other considerations:
• High index of clinical suspicion prior to amniotomy is needed since not all cases are diagnosed by ultrasound before birth [15]. This is particularly true in monochorionic diamniotic twins and some IVF conceived twins or IVF conceived higher order multiples.
• Type II Vasa Previa (from bilobed or succenturiate lobe placenta ) has been successfully treated with in utero laser. [60]
• Newer methods of detecting fetal hemoglobin have been described, which could aid early diagnosis of clinical vasa previa. [61]
Vasa Previa: Imaging Considerations
Vasa previa occurs when sub-membranous fetal vessels cross the internal cervical os.
Three possibilities exist:
1. Velamentous cord insertion occurs with vessels traversing membranes, which cross over or near the internal os.
2. Bi-lobed placenta is present and fetal vessels traverse membranes from one lobe to the other lobe and cross over the internal os or near the internal os.
3. History of mid-trimester placenta previa occurs, the marginal placental mass is absorbed and there is membranous fetal vessel exposure over or near the internal os.
Scanning observations:
1. On transabdominal gray scale, echogenic parallel or circular lines may appear near the internal cervical os, which likely represent the umbilical vessels.
2. Carefully observe cord insertion site, particularly if there is placental implantation in the lower one third of the uterus. [62]
3. Assess for the possibility of an accessory lobe or a succenturiate lobe.
4. Distinguish between marginal cord insertion and velamentous cord insertion.
5. Observe the cervical vascular arrangement in patients with the placental margin near the internal cervical os.
Confirmation of the diagnosis:
1. Perform transvaginal ultrasound.
2. Use color Doppler to identify fetal vessels.
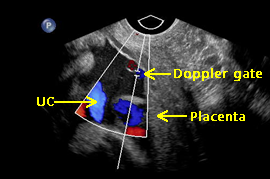
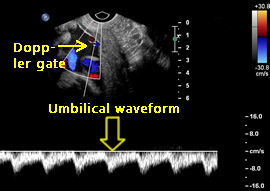
3. Place pulsed Doppler gate within fetal vessels and confirm fetal origin on Doppler velocimetry.
Pitfalls in the diagnosis:
1. The umbilical cord may be presenting in the lower uterine segment and near the cervix, but no sub-membranous vessels are traversing the internal cervical os.
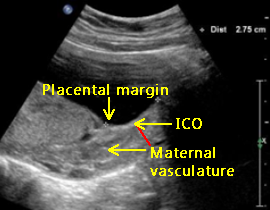
2. Placental implantation near the internal cervical os may exhibit maternal veins.
3. Maternal cervical vessels near the internal cervical os can be observed with color Doppler and can be mistaken for fetal vessels.
In all of the cases cited above, pulsed Doppler velocimetry will distinguish maternal vasculature from fetal vasculature.
Vasa Previa: Images
Vasa Previa, Patient 1


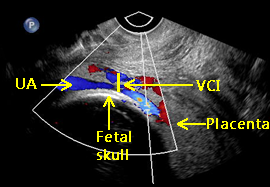
Above. Patient 1. 21 2/7ths weeks. 2-D gray scale. Longitudinal view. PL (placenta) demonstrating velamentous CI (cord insertion). Note AL (accessory lobe), CR (cervical region), and maternal BL (bladder).


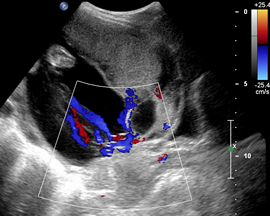
Above. Patient 1 (continued). Color Doppler image demonstrating velamentous CI (cord insertion).


Above. Patient 1 (continued). Color Doppler image, again demonstrating VCI (velamentous cord insertion). Again, note AL (accessory lobe) and CR (cervical region).
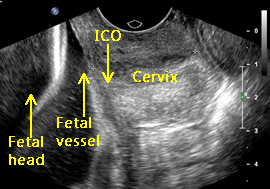

Above. Patient 1 (continued). Transvaginal ultrasound. 2-D gray scale. Sagittal view demonstrating ICO (internal cervical os). A sub- membranous fetal vessel is identified near the ICO.


Above. Patient 1 (continued). Transvaginal ultrasound. Sagittal view. Color Doppler image confirming the fetal vessel seen in the gray scale view.


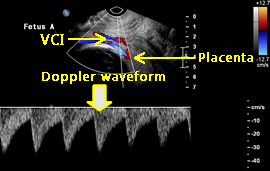
Above. Patient 1 (continued). 3rd trimester. Transvaginal ultrasound color Doppler image suggests a fetal vessel. Pulsed Doppler velocity waveform confirms the presence of a fetal arterial vessel and substantiates the diagnosis of vasa previa, which was observed following delivery by C-section.
Vasa Previa, Patient 2


Above. Patient 2. 25 weeks. 2-D gray scale. Longitudinal view. Note 2 separate placental masses.


Above. Patient 2 (continued). Color Doppler image demonstrating VCI (velamentous cord insertion). Note the AL (accessory lobe) and the apparent cord insertion site between the anterior placenta and the accessory lobe.

Above. Patient 2 (continued). Color Doppler image demonstrating VCI (velamentous cord insertion). Note the cord insertion site is near the cervical region.

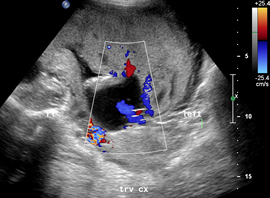
Above. Patient 2 (continued). Color Doppler image with transverse view of the cervix demonstrating sub-membranous insertion of fetal vessel near cervix.


Above. Patient 2 (continued). Transvaginal ultrasound view, color Doppler image confirming the fetal vessels inserting near and crossing over the ICO (internal cervical os). Pulsed Doppler confirmed the fetal origin of the vessels.
Vasa Previa, Patient 3


Above. Patient 3. 29 2/7 weeks. 2-D gray scale. Transverse view. Note 2 separate placental masses with apparent cord insertion into the margin of the anterior placenta.
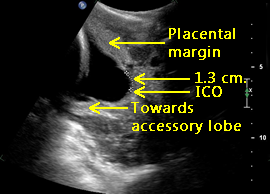

Above. Patient 3 (continued). 2-D gray scale. Longitudinal view of lower uterine segment and cervix. Note that the leading edge of the main placental mass is 1.3 cm from the ICO (internal cervical os).


Above. Patient 3 (continued). Transvaginal ultrasound, 2-D gray scale image suggesting fetal vessels are crossing the ICO (internal cervical os).


Above. Patient 3 (continued). Transvaginal ultrasound view, color Doppler image. Fetal vessels connect the accessory placental lobe to the placenta, while crossing at or near the internal cervical os.


Above. Patient 3 (continued). Transvaginal ultrasound view, color Doppler image. Pulsed Doppler ultrasound confirms that the vessels in question are fetal vessels crossing at or near the internal cervical os.
Vasa Previa, Patient 4


Above. Patient 4. Twin gestation with posterior placenta and suspected VCI (velamentous cord insertion). Transvaginal ultrasound, 2-D gray scale demonstrates the margin of the placenta to be near the cervix and the velamentous cord inserting into the placental margin near the cervix.

Above. Patient 4 (continued). Transvaginal ultrasound view, color Doppler image demonstrates the VCI (velamentous cord insertion) into the placental margin and one of the UA (umbilical arteries). The sub-membranous fetal vessels are crossing the cervix near the internal cervical os.

Above. Patient 4 (continued). Transvaginal ultrasound view, color Doppler image. The pulsed Doppler ultrasound waveform confirms the presence of a fetal arterial vessel at or near the internal cervical os.
Vasa Previa versus Umbilical Cord, Patient 5
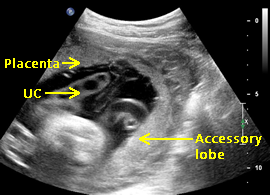

Above. Patient 5. 2-D gray scale. Transverse view. Note 2 separate placental masses with an anterior placenta and a possible accessory lobe. There are multiple free loops of UC (umbilical cord).
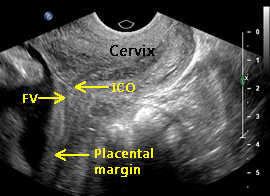

Above. Patient 5 (continued). Transvaginal ultrasound, 2-D gray scale demonstrates the margin of the placenta to be near the cervix. There is the possibility of a FV (fetal vessel) on gray scale. Alternatively, the fetal vessel could represent a retro-placental vascular space of maternal origin.


Above. Patient 5 (continued). Transvaginal ultrasound view, color Doppler image demonstrates a FV (fetal vessel) near the ICO (internal cervical os) and a loop of UC (umbilical cord). The goal is to demonstrate the difference between a free loop of umbilical cord and a sub-membranous fetal vessel over the ICO.

Above. Patient 5 (continued). Transvaginal ultrasound view, color Doppler image. The pulsed Doppler gate should be placed when there is a simultaneous view of the internal cervical os on transvaginal ultrasound. In this image, the placement is not correct.

Above. Patient 5 (continued). Transvaginal ultrasound view, color Doppler image. Again, the pulsed Doppler gate should be placed when there is a simultaneous view of the internal cervical os on transvaginal ultrasound. While the waveform is fetal in origin, the possibility of an umbilical cord vessel versus a sub-membranous vessel over the os cannot be delineated in this view.


Above. Gray scale image, longitudinal view demonstrates the UC (umbilical cord) and the ICO (internal cervical os). Transvaginal ultrasound with color Doppler and pulsed Doppler is necessary to define vasa previa.

Above. 2-D gray scale demonstrating the ICO (internal cervical os) and the placenta near the ICO. Marginal placental vascular structures are common in this location, and pulsed Doppler may demonstrate maternal arterial or venous structures.


Above. Pulsed Doppler demonstrating a vessel near the cervix with a rate of 75 bpm consistent with maternal origin.
Vasa Previa: Video
Above. Vasa previa. 2-D gray scale demonstrating the ICO (internal cervical os) and sub-membranous fetal vessel. This finding requires transvaginal ultrasound with color Doppler. Suspected fetal vessels should be imaged in relationship to the ICO, and pulsed Doppler waveforms should verify fetal origin.
Above. Vasa previa. 2-D gray scale demonstrating flow within fetal vessel near the placental margin and the ICO (internal cervical os).
Above. VCI (velamentous cord insertion) near the cervical region. Again, this finding requires transvaginal ultrasound with color Doppler. Suspected fetal vessels should be imaged in relationship to the ICO, and pulsed Doppler waveforms should verify fetal origin.
Above. VCI (velamentous cord insertion) near the internal cervical os, a risk factor for vasa previa.
Above. Vasa previa. Transvaginal color Doppler scan demonstrating FV (fetal vessel) crossing the internal cervical os. Pulsed Doppler waveform confirmed fetal origin.
Above. Vasa previa. Transvaginal color Doppler scan demonstrating FV (fetal vessel) crossing the ICO (internal cervical os). These vessels traverse sub-membranously between the accessory placental lobe and the placenta.
Above. Twin gestation. VCI (velamentous cord insertion) near the cervix, a risk factor for vasa previa.
Above. Same patient as above. 2-D grayscale transvaginal ultrasound demonstrating VCI (velamentous cord insertion) into the margin of the placenta adjacent to the ICO.
Chorioangioma: Information
Page Links: Definition, Pathology, Risk Factors, Etiology, Prenatal Outcome, Neonatal Outcome, Treatment, References
Introduction
Chorioangiomas are benign vascular tumors of the placenta. Larger lesions can be seen on ultrasound and color Doppler can define their size and extent. Larger tumors can be associated with fetal morbidity, as the tumors act as peripheral arteriovenous shunts and cause high output cardiac failure. Lesions can be clinically associated with changes in amniotic fluid volume, fetal anemia, and fetal growth. Various strategies have been proposed for prenatal treatment.
Definition and Incidence of Fetal Chorioangioma

Chorioangioma (CA) is the most common benign, vascular, non-trophoblastic tumor of the placenta. [63] The incidence is .05 to 1.3% of placentas. [1]
Pathology of Chorioangioma

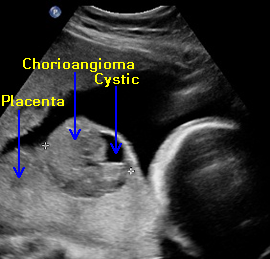
Chorioangiomas most often are small (< 0.5 cm), incidental findings on pathologic examination of the placenta. When larger, these lesions can be seen with ultrasound and may have significant clinical consequences. CAs may be nodular or multinodular and are located on the chorionic plate, protruding toward the fetus. Histologically, these lesions show nonspecific findings of trophoblastic hyperplasia similar to partial moles. [64]

Other rare forms of vascular placental tumors include chorangiosis (CH) and chorangiomatosis (CM). These are villous capillary (VC) lesions that may also be related to hypoxemia, and each of these rarer forms of vascular tumors may have specific clinical associations. [2] Chorangiosis has a relatively high association with stillbirth [65] and occurs with a different gestational age distribution compared to other placental vascular lesions. [66]
Risk Factors
Risk factors include a linear increase with maternal age, hypertension, diabetes, and female gender. [67]
Etiology
Increased growth factor expression may play a part in chorioangioma formation. [68] Others report potential angiogenic precursors, which might play a role in tumor formation. [69] Genes that lie in certain DNA regions may be a part of the pathogenesis of chorioangioma. [70]
Prenatal Outcome of Fetal Chorioangioma

Larger chorioangiomas can result in the poor fetal outcome. In the angiomatous type of chorioangioma, the tumor within the vascular bed acts as an arteriovenous shunt that can induce hemodynamic changes in the fetus [71] resulting in high output cardiac failure and fetal hydrops. A second mechanism is through a functional empty space due to the tumor.
As a result of these mechanisms, adverse fetal events can occur. Complications include: polyhydramnios, preterm birth, fetal growth restriction, anemia, fetal congested heart failure, non-immune fetal hydrops, and an increase in perinatal mortality. [9] Microangiopathic thrombocytopenia may also result.
Poor outcome is reported in over 50% of the cases. In 9 cases of chorioangioma detected in singletons, 5 were associated with pregnancy complications; of the 5, all had abnormalities of amniotic fluid volume; 2 were associated with growth restriction, and 1 with non-immune hydrops. In addition, 44% delivered before 35 weeks. [72]
Chorioangioma’s Neonatal Outcome


The presence of chorioangioma in the placenta results in neonatal consequences similar to those seen antenatally. Newborns can present with severe anemia, thrombocytopenia, heart failure, and growth restriction. Cerebral embolism has been reported with diffuse chorioangiomas that occurred before birth but resulted in neonatal neurological compromise. [73]
In addition, placental vascular tumors can occur simultaneously with infantile hemangiomas. [74] Chorioangioma is also reported in association with multiple diffuse cutaneous and liver angiomatosis. [75] Others have described multiple diffuse resolving neonatal hemangiomatosis after a pregnancy complicated by placental chorioangioma. These vascular tumors that occur in the placenta and in the neonate may share a common histopathology. [12]
Treatment of Fetal Chorioangioma

A number of potential treatment options for chorioangioma have been reported. These include: fetal transfusion, fetoscopic devascularization, embolization, and injection with absolute alcohol. [76]
1. Fetal alcohol ablation of a feeding vessel was performed successfully in a patient with a large chorioangioma accompanied with polyhydramnios and fetal hydrops, although delivery occurred at 32 weeks. [77] Another report of alcohol injection resulted in a 28 week delivery. [78]
2. Laser directed at the feeding vessel and interstitial laser is reported with variable success in a small number of patients. [79], [80], [81]
3. Indomethacin to treat associated polyhydramnios was thought to be successful in delaying delivery for 3 weeks. [82]
4. Finally, peak systolic velocity measurements of the middle cerebral artery define anemia and guide fetal transfusion therapy. [83]
Chorioangioma: Imaging Considerations
Grayscale

Imaging options include grayscale, color Doppler, and 3-D power Doppler. Chorioangiomas are of various sizes and shapes. On grayscale, they are well-circumscribed and protrude from the fetal surface of the placenta, and the echotexture is different from normal placental texture. The average size of a placental chorioangioma is 6.5 cm, and they range from 4 to 13 cm. [84]
Color Doppler
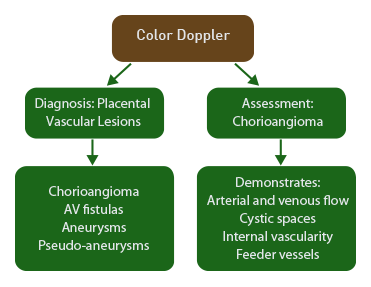
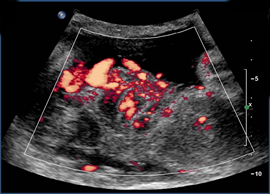
Color Doppler ultrasound is an important component in evaluating solid placental masses seen on gray scale. [85] It is an effective modality in a number of placental abnormalities, including chorioangiomas, arteriovenous fistulas, true aneurysms, and pseudo-aneurysms. Chorioangiomas demonstrate both arterial and venous flow and contain cystic spaces that produce color signals. [86] Both internal vascularity and the presence of a large feeding vessel confirm the diagnosis. [1]

The degree of vascularization determines the outcome for chorioangiomas. Those with a high degree of vascularization have a higher likelihood of polyhydramnios, fetal growth restriction, and fetal hydrops. [87] Others confirm that flow within the mass is a distinguishing feature for chorioangioma and that these cases are often accompanied by polyhydramnios and/or premature labor. [88] A demonstrated reduction over time for chorioangioma intramural blood flow is associated with improved outcome. [89] Those that are avascular are unlikely to be associated with complications. [4] Depending upon size, lesions that are not primarily within the placenta (retro-placental or subchorionic hematomas) have better outcomes compared to chorioangiomas. [2]
3-D Color Power Doppler

Three-dimensional power Doppler ultrasound depicts architecture and flow within chorioangiomas. [6] The architectural information includes the continuity, curvature and surface characteristics of the tumor. [90] Finally, 3-D ultrasound may provide information about vascular volume. [91]
Chorioangioma: Images
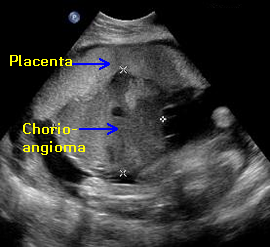

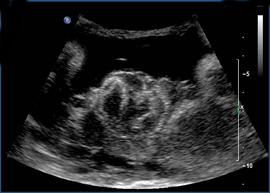
Above. Chorioangioma. Patient 1. 28 weeks gestation, large placental mass on gray scale ultrasound. Note the difference in texture between the placenta and the chorioangioma which measures 10.3 cm X 9.7 cm.
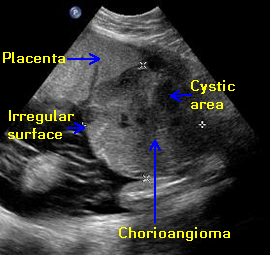

Above. Chorioangioma. Patient 1. Chorioangiomas typically protrude towards the fetal side of the placenta. The outside contour of the mass is irregular and there are cystic areas within the tumor.


Above. Chorioangioma. Patient 1. Color power Doppler confirms the moderate vascularity of the mass.
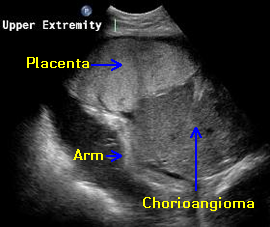

Above. Chorioangioma. Patient 1. Note the size of fetal arm in relationship to the 10.9 cm placental mass.


Above. Chorioangioma. Patient 1 (continued). Because the chorioangioma is acting as a peripheral arteriovenous malformation, signs of cardiac failure with cardiomegaly and pericardial effusion are present.


Above. Chorioangioma. Patient 1 (continued). The fetus developed other signs of hydrops including scalp edema.


Above. Chorioangioma. Patient 1 (continued). Other signs of fetal hydrops included abdominal ascites.


Above. Chorioangioma. Patient 1 (continued). Polyhydramnios developed with the subsequent onset of premature labor. Delivery occurred at 28 2/7 weeks gestation with neonatal survival. Pathology evaluation of the placenta confirmed chorioangioma.

Above. Chorioangioma. Patient 2, 29 2/7 weeks gestation with placental mass. The mass measures 5.2 cm in diameter. Note the cystic area within the mass which is a common finding.


Above. Chorioangioma. Patient 2 (continued). Color Doppler flow demonstrates moderate vascularity. Note feeder vessel from the placenta and the cystic area within the chorioangioma. Clinical findings included pleural effusion and polyhydramnios.


Above. Chorioangioma. Patient 2 (continued). Color Doppler again demonstrates a large feeder vessel from the placenta. Fetal thoracentesis was performed and there was resolution of the pleural effusion. Delivery occurred at 37 weeks gestation and pathology of the placenta confirmed chorioangioma.

Above. Chorioangioma. Patient 3. 2-D gray scale showing a discrete mass (chorioangioma) arising from a posterior placenta.

Above. Chorioangioma. Patient 3 (continued). Note color power Doppler demonstrating the vascularity of the chorioangioma.


Above. Chorioangioma. Patient 3 (continued). Left. Color power Doppler. Chorioangioma is demonstrated with increased vascularity and cystic spaces within the tumor. Right. Fetal heart rate tracing demonstrates non-reassuring fetal status with tachycardia and decelerations.


Above. Chorioangioma. Patient 4, 34 3/7 weeks. No evidence for fetal hydrops, but modest growth restriction is present with the estimated fetal weight at the 14th percentile for gestational age. Note the cystic space with the choiroangioma.


Above. Chorioangioma. Patient 4 (continued). Note the prominent “feeder vessel.” The mass was of small size (5.0 cm).


Above. Chorioangioma. Patient 5. Note measurement of the 7.6 cm chorioangioma.
Chorioangioma: Video
Above. Chorioangioma. 2-D gray scale with sagittal view of placenta. Large chorioangioma (10 cm) with cystic spaces as part of the vascular tumor.
Above. Chorioangioma. 2-D gray scale. Again, chorioangioma with cystic spaces as part of the vascular tumor.
Above. Chorioangioma. Color Doppler. Color flow demonstrates the vascular pattern within the chorioangioma and the apparent placental insertion of the umbilical cord near the tumor. Again, note cystic spaces within the mass.
Above. Chorioangioma. Color Doppler. Again, the settings with the color Doppler demonstrate the vascularity of this large chorioangioma, which was associated with fetal hydrops, polyhydramnios, and spontaneous premature delivery.
Above. Chorioangioma. Color Doppler. The chorioangioma is demonstrated. The tumor measures 5 cm and the placenta is demonstrated separately with a “feeder vessel” arising from the placenta.
Above. Chorioangioma. Color Doppler. The chorioangioma is again demonstrated. Note the vascular pattern within the placenta and the well-defined feeder vascular structures.
References
-
Abstract: PMID: 11997676 -
Abstract: PMID: 17012465 -
Abstract: PMID: 12380606 -
Abstract: PMID: 15672024 -
Abstract: PMID: 15861413 -
Abstract: PMID: 16212842 -
Abstract: PMID: 16513243 -
Abstract: PMID: 14962795 -
Abstract: PMID: 15036707 -
Abstract: PMID: 12857557 -
Abstract: PMID: 12541219 -
Abstract: PMID: 15192293 -
Abstract: PMID: 16513243 -
Abstract: PMID: 15229003 -
Abstract: PMID: 17826417 -
Abstract: PMID: 11207150 -
Abstract: PMID: 18191809 -
Abstract: PMID: 2088244 -
Abstract: PMID: 18226129 -
Abstract: PMID: 18271885 -
Abstract: PMID: 18702104 -
Abstract: PMID: 17960788 -
Abstract: PMID: 17355267 -
Abstract: PMID: 12850613 -
Abstract: PMID: 2106217 -
Abstract: PMID: 8437776 -
Abstract: PMID: 3920264 -
Abstract: PMID: 2677693 -
Abstract: PMID: 3299486 -
Abstract: PMID: 8756935 -
Abstract: PMID: 15042008 -
Abstract: PMID: 3307354 -
Abstract: PMID: 6605073 -
Abstract: PMID: 3538831 -
Abstract: PMID: 6974999 -
Abstract: PMID: 7054842 -
Abstract: PMID: 11997676 -
Abstract: PMID: 17012465 -
Abstract: PMID: 12380606 -
Abstract: PMID: 15672024 -
Abstract: PMID: 6605073 -
Abstract: PMID: 3538831 -
Abstract: PMID: 11222189 Derbala Y, Grochal F, Jeanty P. Vasa previa. Journal of Prenatal Medicine. 2007;1(1):2-13. -
Abstract: PMID: 14619643 Shamas AG, Kambhapati L, Abu-Ghazza O, Dabbagh Z, Abdul-kadirbi R. Prenatal diagnosis of velamentous cord insertion and vasa praevia using ultrasound and magnetic resonance imaging: a case report. Ultrasound. 2008;16(1):15-17. -
Abstract: PMID: 15498919 -
Abstract: PMID: 1733612 -
Abstract: PMID: 17497747 -
Abstract: PMID: 17497747 -
Abstract: PMID: 16858739 -
Abstract: PMID: 17556824 -
Abstract: PMID: 17477103 -
Abstract: PMID: 14963081 -
Abstract: PMID: 25491755 -
Abstract: PMID: 10725492 -
Abstract: PMID: 11169317 -
Abstract: PMID: 16903253 -
Abstract: PMID: 15121568 Allen MH, Bornick PW, Kontopoulos EV, Quintero RA. In utero laser treatment of type II vasa previa. The Journal of Maternal-Fetal & Neonatal Medicine. 2007;20(12):47-851. -
Abstract: PMID: 16797824 -
Abstract: PMID: 16858739 -
Abstract: PMID: 15022059 -
Abstract: PMID: 10987255 -
Abstract: PMID: 16208478 -
Abstract: PMID: 14989498 -
Abstract: PMID: 12747233 -
Abstract: PMID: 12747234 -
Abstract: PMID: 12852866 -
Abstract: PMID: 17203486 -
Abstract: PMID: 12364888 -
Abstract: PMID: 14672481 -
Abstract: PMID: 16737029 -
Abstract: PMID: 17937433 -
Abstract: PMID: 14663833 -
Abstract: PMID: 15085884 -
Abstract: PMID: 12078971 -
Abstract: PMID: 17228160 -
Abstract: PMID: 19156708 -
Abstract: PMID: 14607052 -
Abstract: PMID: 15736199 -
Abstract: PMID: 11776505 -
Abstract: PMID: 16969001 -
Abstract: PMID: 12164576 -
Abstract: PMID: 11169350 -
Abstract: PMID: 11796897 -
Abstract: PMID: 11005112 -
Abstract: PMID: 11169351 -
Abstract: PMID: 15287061 -
Abstract: PMID: 14671412 -
Abstract: PMID: 16389043
44
46
60