 Search
Search
Umbilical Cord: Normal and Abnormal
The following are the topics covered in this course:
Normal Umbilical Cord
Single Umbilical Artery
Umbilical Vein Varix
Marginal Cord Insertion
Velamentous Cord Insertion
Umbilical Cord Cysts
Normal Umbilical Cord
Page Links: Umbilical Cord Development, Umbilical Cord Blood Flow, References-End

The critical embryological times are at 24 to 25 days, the beginning of the 6th week, and during the 10th week. At 24 to 25 days, the abdominal wall forms and the yolk sac and its connections to the midgut are established. The intestines project into the cord at the beginning of the 6th week, and during the 10th week, the intestines return to the abdomen. [1]


Graphic by John D’Agostino (modified).
Above left. The umbilical cord (UC) is derived from the stalk of the yolk sac, while the yolk stalk fuses with the omphalomesenteric duct (OMD). [1] The out pouching of bladder (Bl) forms the urachus (U). The urachal extension into the cord forms the allantois (Al). The allantoic vessels become the umbilical vessels. [1]
Above right. This is a transverse view of the fetal abdomen at about 9 weeks showing projection of the midgut into the umbilical cord insertion site.
Above. From the 6th through the 9th week, the developing intestines project into the umbilical cord insertion site. [1]
Umbilical Cord Blood Flow


Above. The normal umbilical cord has 2 umbilical arteries (UA) and 1 umbilical vein (UV). The umbilical arteries are branches of the fetal internal iliac arteries. They bring deoxygenated blood from the fetus to the placenta. Each artery courses around the fetal bladder and enters the umbilical cord at the abdominal CI (cord insertion site). The umbilical vein brings oxygenated blood from the placenta to the fetus and enters the fetal liver at the abdominal cord insertion site. About 50% of the umbilical venous blood is shunted through the ductus venosus to the inferior vena cava before entering the right atrium.

Above. Longitudinal gray scale view. The umbilical vein (UV) enters the abdominal cord insertion site. The LPV (left portal vein) receives well oxygenated blood from the umbilical vein and continues to the DV (ductus venosus) and then to the IVC (inferior vena cava) and right atrium.
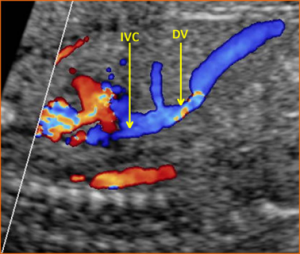
Above. Longitudinal view. Color Doppler. The umbilical vein enters the fetal liver. Note the flow through the ductus venosus (DV) and inferior vena cava (IVC) with well oxygenated blood entering the right atrium.
Normal Umbilical Cord: Imaging Considerations

All aspects of umbilical cord development are complete by 10 to 11 weeks gestation. [2] The normal umbilical cord is shown with its placental insertion site and is covered by a glistening layer of amnion. The average length is 55 cm and it may be spiraled or helical. [3]
Two dimensional images of umbilical cord should include the following:
- Gray scale transverse views.
- Placental cord insertion site.
- Abdominal cord insertion site.
- Color Doppler transverse views.
- Color Doppler arterial flow around the fetal bladder.
Normal Umbilical Cord: Images

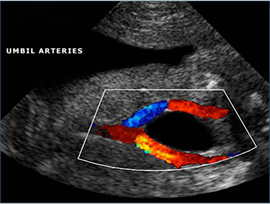
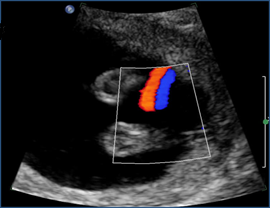
Above. Color Doppler image. Normal umbilical artery flow with 2 umbilical arteries coursing around the fetal bladder.
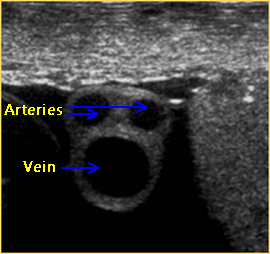

Above. 2-D gray scale and transverse view of the umbilical cord demonstrating 2 arteries of equivalent size and the larger umbilical vein.


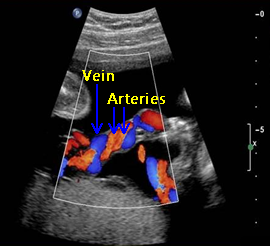
Above. Color Doppler image. Transverse view of a normal umbilical cord demonstrating 2 arteries and 1 vein.
Above. Color Doppler image. Longitudinal view demonstrating 2 arteries and 1 vein.
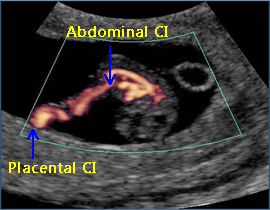

Above. Color power Doppler demonstrating both the placental cord insertion site and the abdominal cord insertion site. The umbilical cord (UC) diameter increases in size from 8 to 15 weeks. The UC diameter correlates with [4]: gestational age (GA), crown rump length (CRL), and biparietal diameter (BPD). By the end of the first trimester, there is normal blood flow in the midgut area.


Above. 2-D gray scale demonstrating abdominal cord insertion site. At 18 to 23 weeks, the umbilical cord diameter measured at the insertion into the fetal abdominal wall correlates with gestational age (GA) and estimated fetal weight (EFW). [5]


Above. 2-D gray scale. Transverse view of the fetal abdomen. Note the UC (umbilical cord) insertion at the fetal abdomen with a view of the UV (umbilical vein) with its entry into the fetal liver. At 24-39 weeks, the umbilical cord cross sectional area measured at insertion into fetal abdominal wall correlates with [6]: gestational age (GA).


Above. 2-D gray scale. Transverse view of the fetal abdomen. Again, note the umbilical cord insertion into the fetal abdomen. The UA (umbilical artery) and the UV (umbilical vein) are noted.


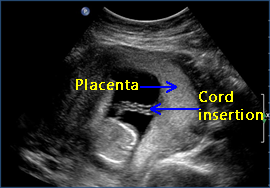
Above. 2-D gray scale. Normal umbilical cord insertion into the placenta. The placenta is posterior and the vascular pattern within the placenta suggests a 3-vessel cord.
An umbilical cord diameter of less than the 5th percentile for gestational age correlates with spontaneous miscarriage and preeclampsia. [3] Umbilical cord diameter and umbilical cord thickness at 14-23 weeks [7] and 18 to 23 weeks [8] respectively correlate with the presence of fetal aneuploidy.
Above. 2-D gray scale demonstrating normal umbilical cord insertion into a laterally implanted placenta.

Above. Color Doppler image. Note central cord insertion site into the placenta. Umbilical cord with large cross sectional area at > 34 weeks correlates with the presence of fetal macrosomia at > 4000 grams and > 4500 grams. [9] In that study, the correlation with macrosomia was best when an umbilical cord area exceed 250 mm2 and the abdominal circumference was > 9th percentile for gestational age. The umbilical artery’s discordant size does not affect outcome. The average luminal size variation is 13.1%. [10]


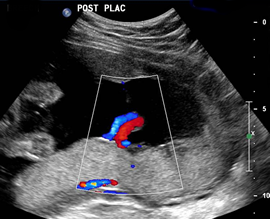
Above. Color Doppler image. Note the anterior placenta with central cord insertion. The umbilical vein cross sectional area at > 20 weeks and reduced Wharton’s jelly also correlates with perinatal death and NICU admissions. [11]
Excessively long umbilical cords occur and are associated with a variety of adverse perinatal events. [12] Seventy centimeters is usually considered excessive umbilical cord length.
Essential ultrasound views for every ultrasound exam include a 3-vessel view and cord insertion into the fetal abdomen. [13],[14]
Three vessel confirmation can be obtained by demonstrating 2 umbilical arteries around the fetal bladder or a transverse view of the cord in 2-D or color Doppler.
Demonstrating a normal cord insertion into the anterior abdomen is the other essential view and can be performed with the use of gray scale or color Doppler imaging.
Summary
1. Essential elements for a standard ultrasound examination include demonstration of: A). the number of fetal vessels and B). the cord insertion into the fetal abdomen.
2. The normal umbilical cord is coiled or helical, covered by a glistening layer of amnion and Wharton’s jelly, and measures approximately 50 cm in length. [2]
3. The first trimester cord increases in size from 8 to 15 weeks. The umbilical cord diameter correlates with gestational age, crown rump length, and biparietal diameter. [3]
4. At 18 to 23 weeks, the umbilical cord diameter correlates with gestational age and estimated fetal weight. [4]
5. At 24-39 weeks, the umbilical cord cross sectional area measured at insertion into fetal abdominal wall correlates with gestational age. [5]
6. Areas of investigation which may hold promise for clinical care include:
a). Umbilical cord diameter, which correlates with
spontaneous miscarriage, preeclampsia, and aneuploidy [6],[7]
b). Umbilical cord cross sectional area, which correlates with fetal macrosomia at > 4000 grams and > 4500 grams. [8]
Normal Umbilical Cord: Video
Above. Color Doppler video. Central cord insertion into the posterior placenta.
Single Umbilical Artery
Page Links: Definition/Development, Incidence, Outcomes, Malformations, Aneuploidy, Fetal Growth Restriction, References
Definition/Development
Normally, the umbilical cord contains 2 umbilical arteries and 1 umbilical vein. A single umbilical artery (SUA) is also known as 2-vessel cord.
An isolated single umbilical artery is defined as the presence of a single umbilical artery without:
• known fetal anomaly
• malformation
• aneuploidy or growth restriction

Umbilical cord facts:
1. The 4th and 5th week after fertilization are key times for umbilical artery development. [15],[16]
2. Fused umbilical arteries are distinct from SUA and occur in a small number of cases. [17]
3. An isolated single umbilical artery carries twice the blood flow compared to the two umbilical arteries in a 3-vessel cord. [18]
Incidence

Above. The incidence of single umbilical artery depends upon the study population. The incidence is generally lower in populations of patients from antenatal ultrasound studies [19],[20] compared to pathological studies. [21],[22]
Outcomes
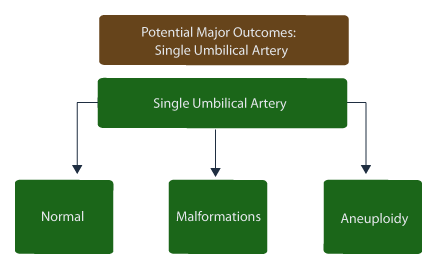
Above. Potential major outcomes include isolated single umbilical artery, major or minor malformations, fetal aneuploidy, and possibly, fetal growth restriction.

Above. Outcomes for SUA in ultrasound ascertained cases report fewer malformations and chromosomal abnormalities compared to pathologically determined cases (cases determined from placentas and pathology records). [6],[7]

Above. Cases determined from placenta and pathology records report higher numbers of malformations and chromosomal abnormalities. [7]

Above. The percent of normal subjects with a diagnosis of SUA is higher in the ultrasound ascertained cases (85%) [6] compared to studies from pathology records (63%). [7]
Malformations
These associations are not unexpected and may differ further from ascertainment based upon infants or neonates.

Above. The presence of single umbilical artery is more likely in neonates with malformations present than in neonates with malformations absent (2.29% versus 1.03%).

Above. The most common malformation associated with SUA is cardiovascular. [23] Fetal genitourinary defects are generally minor and self-limiting. [24] In addition, other malformations are listed that occur more frequently with SUA compared to a normal 3-vessel cord. [11] Finally, an association is reported among neonatal skin angiomas. [25]
Aneuploidy
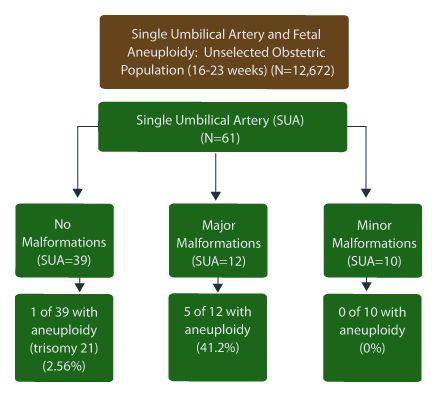
Single umbilical artery is more likely to be associated with fetal aneuploidy if major malformations are present than if major malformations are absent. In the absence of malformations, fetal aneuploidy occurs in less than 3% of subjects [26] and other studies confirm this observation. [27]
Other reports suggest an association between isolated SUA and fetal aneuploidy at 1 in 24. (4%). [28] In a retrospective review of 5987 ultrasounds performed at 20 weeks, no aneuploidy was found in the absence of other associated findings. [6]

Above. In mid-trimester pre-amniocentesis studies, the rate of fetal aneuploidy is significantly greater in fetuses with single umbilical artery compared to fetuses with normal 3-vessel cord. (18.6% versus 5.3%), P < .001. [13]
At 11 to 14 weeks, the umbilical cord diameter is smaller in chromosomally abnormal fetuses compared to those with normal chromosome count. [29] SUA is reported in 3.3% of fetuses with normal chromosomes. [30] At 11 to 14 weeks, SUA is present in 11.4% of fetuses with Trisomy 21; in 77.8% of fetuses with Trisomy 18; and in 9.5% of fetuses with other chromosomal defects. [16]
Fetal Growth Restriction

Above. The relationship between SUA and fetal growth restriction is controversial, and likely depends upon the population which is studied.
In longitudinal studies based on antenatal ultrasound results, the percent of fetuses with growth restriction and single umbilical artery and the percent of fetuses with growth restriction and 3-vessel umbilical cord were not different. [31],[32]
Other ultrasound series of growth in pregnancies with SUA report a small number of fetuses (2.9%) affected with growth restriction. [5] Again, these findings may be population based.
Other reports suggest fetuses with SUA weigh less at birth [8] or are at risk for associated fetal growth restriction. [33]
In unselected populations, fetal growth restriction with or without malformations is reported in a relatively high proportion of cases. [14]
In summary, the relationship between SUA and growth restriction depends upon patient selection. In fetuses without aneuploidy or structural malformations, the incidence of growth restriction is low, while the incidence of growth restriction is higher in fetuses affected with these abnormalities.
Single Umbilical Artery: Imaging Considerations
1. In 2-D gray scale, observe the umbilical cord in transverse view.
2. In transverse view, 2 vessels are observed, 1 artery and 1 vein.
3. Apply color Doppler in transverse view, and again 2 vessels are identified.
4. The single umbilical artery in the transverse view is typically larger than that seen in the transverse view of a 3-vessel cord.
5. With a single umbilical artery, Color Doppler in a longitudinal segment of cord demonstrates 2 consistent single vessels.
6. Apply color Doppler scan to the fetal pelvis with a transverse view of the bladder. A single artery coursing around the bladder instead of 2 arteries is observed. Over two thirds of the time, the left umbilical artery is absent.
Single Umbilical Artery: Images


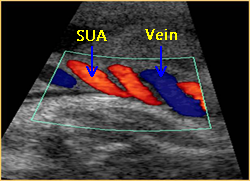
Above. 2-D gray scale view. Transverse of an umbilical cord demonstrating SUA (single umbilical artery); 2-vessel cord with UA (umbilical artery) and UV (umbilical vein). Above. 2-D gray scale view. Oblique view of the umbilical cord demonstrating a SUA (single umbilical artery) and the umbilical vein.

Above. Color Doppler. A continuous longitudinal view demonstrates a SUA (single umbilical artery).

Above. Color Doppler. A continuous oblique view demonstrates a SUA (single umbilical artery).
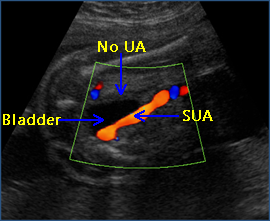

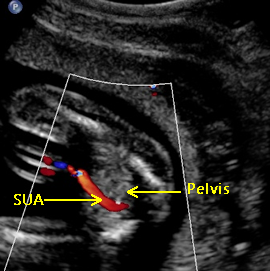
Above. Color Doppler of the fetal pelvis with a transverse view of the bladder illustrating 1 UA (umbilical artery) coursing around the bladder instead of 2. The patent umbilical artery can be described as to its laterality (either right or left).


Above. Color Doppler of the fetal pelvis with a transverse view of the bladder illustrating 1 UA (umbilical artery) and the region of the absent UA.

Above. Color Doppler illustrates a view of the fetal pelvis with the bladder empty. This view is suggestive of a SUA (single umbilical artery) but re-scan with a full fetal bladder would confirm the diagnosis.
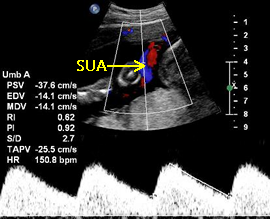

Above. SUA (single umbilical artery) with umbilical artery Doppler waveform. All values are within normal limits for gestational age.
Single Umbilical Artery: Video
Above. 2-D gray scale. Single umbilical artery. Note transverse views of the umbilical cord demonstrate 1 UA (umbilical artery) and 1 UV (umbilical vein ).
Above. 2-D gray scale. Single umbilical artery. Another transverse view of the umbilical cord demonstrates 1 UA (umbilical artery) and 1 UV (umbilical vein).
Above. Color power Doppler view of the fetal pelvis with a transverse view of the bladder. 1 UA (umbilical artery) courses around the bladder. Note the absence of the umbilical artery on the contralateral side.
Above. 2-D gray scale. Single umbilical artery. Note the larger UV (umbilical vein) and the thicker wall of the UA (umbilical artery).
Above. Color Doppler of SUA (single umbilical artery). The umbilical artery is likely in blue and the umbilical vein in red.
Umbilical Vein Varix
Go to top
Page Links: Definition, Diagnosis, Outcome, Other Presentations, Management, References-End
Definition

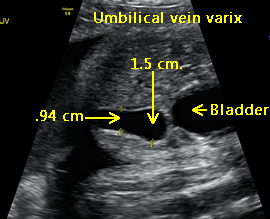
Intra-abdominal umbilical vein varix (UVV) is an aneurysmal dilatation of the umbilical vein. It is associated with an increased fetal death rate and chromosomal abnormalities. UVV is defined as a width of the intra-abdominal portion of the umbilical vein that is > 2 standard deviations for gestational age or any time the width exceeds 9 mm. The varix is both focal and aneurysmal. [34] Approximately 100 cases have been reported to date. [35]
Diagnosis
Elevation of maternal serum alpha-fetoprotein (AFP) and mesenchymal dysplasia have been reported in association with umbilical vein varix. [36]

The umbilical vein varix is typically an ovoid, elongated, fluid-filled mass which is obliquely oriented between the abdominal wall and the edge of liver. [37] Color Doppler confirms venous flow and is diagnostic, while three-dimensional power Doppler (3DPD) ultrasound may be of additional value. [38] Umbilical artery waveform notching may be a predictor for adverse events in instances of umbilical cord abnormalities. [39]
Outcome
Some studies suggest reassuring outcomes. [40] However, other reviews confirm the possibility for adverse events and poor outcome.

In 91 cases, additional anomalies were detected in 31.9%. The most common abnormality was in the cardiovascular system followed by fetal hydrops, and fetal anemia. [41]
Karyotype abnormalities occurred in 9.9% of cases. In summary, 13% of affected fetuses suffered perinatal death and 59.3% of cases had normal outcomes. In cases of isolated umbilical vein varix, intrauterine deaths occurred in 8.1%. Early diagnosis (< 26 weeks) was associated with higher morbidity. [8]

In another study of 25 patients, only 48% had normal outcomes, 13% delivered prematurely, and 35% had structural malformations. [42] In a third study of 26 fetuses, there were other malformations in 19.2%. In addition, 1 of 26 had trisomy 21 and 1 had fetal growth restriction. [43]
Other Presentations

A-V malformations involving the intra-hepatic portion of the umblical vein are reported with Trisomy 21. [44] Umbilical vein varix has been reported in association with Klippel-Trenaunay-Weber (KTW) syndrome (a rare vascular malformation, which includes: soft-tissue hypertrophy, varicose veins, cutaneous hemangiomas, and arteriovenous fistulas). [45] Fetal anemia may be an associated finding. Schistocytic (fragmented red blood cells) anemia can be assessed by peak systolic velocity of the middle cerebral artery. [46] In the newborn, the varix may be confused with an incarcerated umbilical hernia. [47]
Management

Recognition of the varix prenatally allows assessment for other malformations and evidence for karyotype abnormality. If other malformations or makers for aneuploidy are present, karyotype should be offered. If fetal anemia is suspected, peak systolic velocity of the middle cerebral artery should be performed. Some authors recommend close fetal monitoring and delivery at lung maturity. [48] However, intrauterine demise can occur despite close fetal surveillance. [49]
Umbilical Vein Varix: Images


Above. Case 1. Gestational age 33 3/7 weeks. Umbilical vein varix. Transverse scan. An anechoic area within the fetal liver near the umbilical cord insertion site is noted. The diameter is 14 mm.


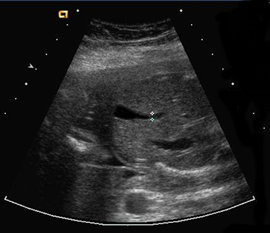
Above. Case 1. Gestational age 33 3/7 weeks. Umbilical vein varix. Oblique scan. this view shows anechoic area within the fetal liver near the umbilical cord insertion site.


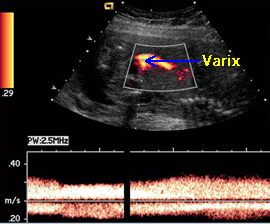
Above. Case 1. Gestational age 33 3/7 weeks. Umbilical vein varix. Color Doppler demonstrates flow and confirms the diagnosis.


Above. Case 1. Gestational age 33 3/7 weeks. Umbilical vein varix. Doppler velocimetry demonstrates mildly pulsatile flow near the varix.


Above. Case 2. 2-D gray scale. Oblique view of the fetal abdomen. Note the bladder and intra-abdominal portion of the hepatic vein with dilatation to 1.1 cm.


Above. Case 2. Color Doppler image of UVV (umbilical vein varix) and UA (umbilical artery). The venous flow confirms the diagnosis.

Above. Case 3. 2-D gray scale. Transverse view of the fetal abdomen. Note the intra-abdominal portion of the umbilical vein which demonstrates moderate dilatation.


Above. Case 3. UVV (umbilical vein varix) measuring 1.6 cm.

Above. Case 4. 2-D gray scale. Oblique view of the abdomen with dilatation of the umbilical vein.


Above. Case 4. Further views confirm dilatation of the umbilical vein of greater than 1.0 cm, suggesting the likelihood of an umbilical vein varix.

Above. Case 4. Color power Doppler confirms venous flow and suggests the diagnosis of umbilical vein varix.
Marginal Cord Insertion
Go to top
Page Links: Definition, Classification/Associations, Frequency, Outcome, Management Issues, Summary, References-End
Definition
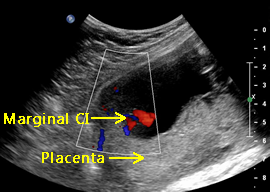
Marginal cord insertion (CI) is defined as the insertion of the umbilical cord within 2 cm of the edge of the placenta.
Classification/Associations
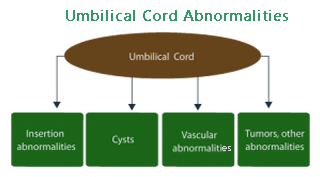
A potential classification is presented for umbilical cord abnormalities. Included are abnormalities of umbilical cord insertions as well as cysts, vascular malformations (single umbilical artery, hemangioma, and hemartoma), and other potential abnormalities such as solid tumors (teratoma).

The abnormalities of umbilical cord insertion include those which are marginal and those which are velamentous (the cord inserts through membranes before placental insertion). The velamentous cord insertion abnormality is a factor in vasa previa when the umbilical vessels cross fetal membranes and the internal cervical os before inserting into the main placental mass.
Frequency
Marginal cord insertion occurs frequently in up to 9.7% in a study of 4677 consecutive placentas. [50]
Outcome
Associations are unlikely between marginal CI and adverse events such as structural defects, growth restriction, or premature labor. [51],[52] In general, the overall outcomes are good.
Management Issues
The major clinical task is to distinguish marginal CI from velamentous cord insertion.
Low cord insertion (lower 1/3 of the uterus), irrespective of whether the insertion is marginal, may be associated with placental malformation and adverse outcomes. [3]
Abnormal cord insertion site may also be associated with reduced coiling of the umbilical cord. [53]
After the birth and before delivery of the placenta, care should be taken to avoid undue cord traction and detachment of the marginal cord insertion site from the placental mass.
Summary
Marginal insertion of the umbilical cord is common (9.7%% in some series). [1]
Generally, outcome is good and is not associated with adverse events such as malformations, growth restriction, or preterm labor. [1],[2]
The antenatal ultrasound detection rate is variable, 93.5% [3] to 54% [4].
Marginal CI should be distinguished from velamentous CI.
Marginal CI in the lower 1/3 of the uterus or near the internal os may pose increased fetal risks such as placental malformation, accessory placental lobe, placental infarction, and emergency Cesarean section. [3]
Marginal Cord Insertion: Images


Above. Gross placental specimen demonstrating a marginal CI (cord insertion) of the umbilical cord. Care should be taken during the 3rd stage of labor since undue traction on the umbilical cord may cause detachment from the placenta and result in retained placenta and/or postpartum hemorrhage.


Above. 2-D gray scale demonstrating a marginal CI (cord insertion) into a posterior fundal placenta.


Above. Color Doppler image demonstrating a marginal CI (cord insertion) into an anterior fundal placenta.


Above. Color power Doppler demonstrating a marginal CI (cord insertion) into an anterior fundal placenta.


Above. Color Doppler demonstrating a posterior placenta in the lower uterine segment with a marginal CI (cord insertion). Marginal CI in the lower 1/3 of the uterus may increase the risk for adverse events.


Above. 2-D gray scale suggests a marginal CI (cord insertion).

Above. Color Doppler. Same patient as above demonstrates color flow, which is confirmatory for marginal CI (cord insertion).


Above. Color Doppler. The cord insertion is marginal. However, the differential diagnosis includes velamentous cord insertion.
Marginal Cord Insertion: Video
Above. Color power. Marginal CI (cord insertion). Note the insertion of umbilical cord in relationship to the placental margin.
Velamentous Cord Insertion
Page Links : Definition/Incidence, Risk Factors, Morbidity, Risk Determinants and Detection, References
Definition/Incidence

Velamentous cord insertion (VCI) is defined as the insertion of the umbilical cord vessels into the fetal membranes prior to their insertion into the main placenta mass. The vessels may also insert into an accessory lobe of the placenta. The incidence of velamentous cord insertion is about 1%. [54] The image above shows twin placenta demonstrating fetal vessels crossing placenta membranes prior to their insertion into the main placental mass.
There is a relationship between VCI and vasa previa. Vasa previa occurs when the velamentous vessels cross the internal opening (internal os) of the cervix or when fetal vessels are exposed to the internal os when crossing between the main placental mass and an accessory lobe of the placenta. These vessels are at risk for compression or rupture when the amniotic membranes rupture before or during labor. Since the fetal blood volume is small, a relatively small amount of blood loss can result in injury or death.
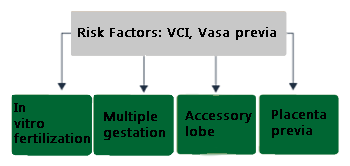
Risk Factors

Risk factors for velamentous CI and vasa previa are similar. [55] There is a higher number of cases in multiple gestation and with in vitro fertilization. The presence of an accessory lobe allows fetal vessels to connect to the main placental mass and if the vessels overlie the internal cervical os, the result is again vasa previa. Trophotropism (the process by which the placenta regresses in the lower uterine segment) may also leave fetal vessels exposed.
Morbidity
Velamentous Cord Insertion: Potential morbidity.
1. As noted above, vasa previa is a potential outcome for velamentous cord insertion. (Incidence: 1 in 2000 to 1 in 5000). [1],[2],[56],[57],[58]
2. Velamentous cord insertions into the lower 1/3 of the uterus are associated with placental malformation, accessory placenta, and placental infarction. [59]
3. Fetal heart rate abnormalities during labor may occur [60] such as fetal heart rate variable decelerations without accelerations. [61]
4. Fetal growth restriction is reported as another possible outcome for VCI. [5]
Risk Determinants and Detection
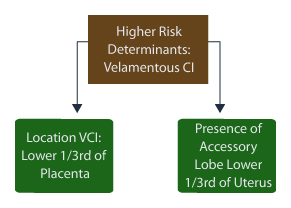
Determinants of risk for velamentous cord insertion depend upon the location of the cord insertion site and the presence of an accessory lobe of the placenta in the lower uterine segment.
Velamentous Cord Insertion: Imaging Considerations
Ultrasound detection rates for velamentous cord insertion (VCI) are about 87% during the second and third trimester. [62] VCI into the posterior placenta is more difficult to detect. [1] At 11 to 14 weeks, detection rates are high and accurate. [63]
The ultrasound detection of VCI reduces the number emergent C-sections [64], and the value of such detection lies in preventing deaths from vasa previa. [65]
The ultrasound approach to velamentous cord insertion and its role in vasa previa includes the following procedures:
1. Attempt to view the internal cervical os by 2-D Gray-scale.
2. Look for echogenic parallel or concentric lines near the cervical os.
3. In the presence of a marginal cord insertion, especially in the lower 1/3 of the uterus, apply color Doppler and ascertain whether fetal vessels course through membranes prior to their insertion into the main placental mass.
4. In 2-D Gray-scale, determine the presence or absence of an accessory lobe and its location in relationship to the internal cervical os. If an accessory lobe is noted, apply color Doppler and record fetal connecting vessels and their location.
5. If fetal vessels are suspected near the internal cervical os, perform transvaginal ultrasound and identify the region of the internal os.
6. Application of color Doppler during the transvaginal ultrasound should demonstrate whether fetal vessels overlie the internal cervical os or are near the internal cervical os.
7. Once a suspected fetal vessel is identified from either VCI or a connection vessel from an accessory lobe, place a Doppler cursor within the vessel to confirm a fetal umbilical waveform.


Above left. Obtain an umbilical artery Doppler recording of the fetal vessel over the internal os. Note fetal heart rate of 148 bpm.
Above right. This measurement confirms fetal origin by defining the fetal heart rate and by demonstrating the typical umbilical artery wave form.
Velamentous Cord Insertion: Images

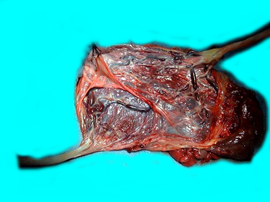
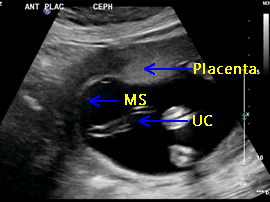
Above. Gross placental specimen: twin placenta. Velamentous cord insertion (VCI) with umbilical vessels coursing through membranes prior to insertion into main placental mass. (UC=umbilical cord; MS=membranous structure; UV=umbilical vessels).


Above. 2-D gray scale. Patient 1. Marginal cord insertion with velamentous insertion. Placental membranes are difficult to see, but the course of the vessels suggest VCI.


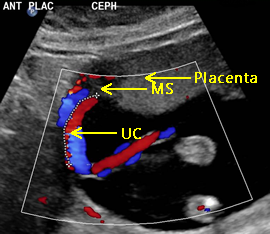
Above. Color Doppler scan. Patient 1 (continued). Marginal cord insertion with velamentous insertion. Placental membranes are difficult to see, but again, the course of the vessels suggest VCI.

Above. 2-D gray scale. Patient 2. Marginal cord insertion with velamentous insertion. Instead of the umbilical cord inserting into the main placenta mass, insertion is towards the amnion/chorion and the uterine wall.

Above. Color Doppler scan. Patient 2 (continued). Marginal cord insertion with velamentous insertion. Instead of the umbilical cord inserting into the main placenta mass, color flow confirms insertion into the dividing membrane prior to insertion into the margin of the placenta.


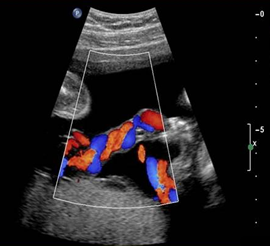
Above. Color Doppler scan. Patient 3. Marginal cord insertion with velamentous insertion. Instead of the umbilical cord inserting into the main placenta mass, color flow suggests insertion into the dividing membrane prior to insertion into the margin of the placenta.


Above. Color power Doppler scan. Patient 4. Marginal cord insertion with velamentous insertion. Instead of the umbilical cord inserting into the main placenta mass, color flow again suggests insertion into the dividing membrane prior to insertion into the margin of the placenta. Direction of flow is shown by the arrow.
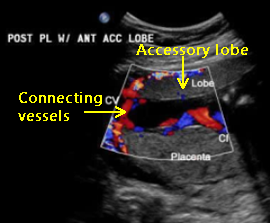

Above. Color Doppler. Patient 5. Accessory placenta on the anterior uterine wall and main placental mass on posterior uterine wall. The cord insertion is to the main (posterior) placental mass and there are fetal connecting vessels between the accessory lobe and the main placenta.
Velamentous Cord Insertion: Video
Above. VCI (velamentous cord insertion) near the cervical region. This finding requires transvaginal ultrasound with color Doppler. Suspected fetal vessels should be imaged in relationship to the ICO, and pulsed Doppler waveforms should verify fetal origin.
Above. VCI (velamentous cord insertion) near the internal cervical os, a risk factor for vasa previa.
Above. Twin gestation. VCI (velamentous cord insertion) near the cervix, a risk factor for vasa previa.
Umbilical Cord Cysts
Page Links: Definition, Classification,
Definition
Cysts of the umbilical cord are defined as thin-walled structures filled with either fluid or mucus. The cysts are located adjacent to or within umbilical cord substance. Umbilical cord cysts are found in approximately 2.1% of all first trimester pregnancies. [66] Most cysts are either at the abdominal cord insertion site or the placental insertion site.
At 7 to 13 weeks gestation, over 20% of fetuses with umbilical cord cysts demonstrate chromosomal or structural defects. [67] However, recent studies suggest a lower likelihood of adverse events and given the limited number of patients studied, fetal prognosis is difficult to predict.
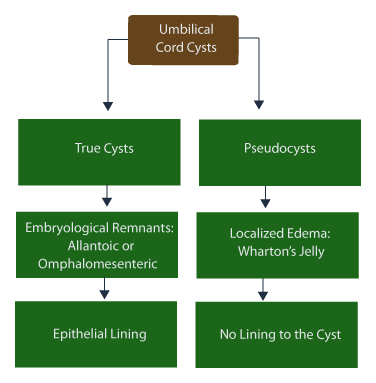
Classification
Umbilical cord cysts are classified as either true cysts or pseudocysts. True cysts are derived from embryological remnants of the omphalomesenteric duct or the allantois. The distinction between the types of cysts depends upon the cyst lining. True cysts arenlined by cuboidal epithelium.

True cysts most often range between 4 mm and 60 mm, but can be smaller. About 20% of any cyst type may be associated with chromosomal aneuploidy. [68] True cysts have associations with other malformations such as omphalocele, patent urachus, hydronephrosis, and Meckel diverticulum.


In a study of 13 patients with pseudocysts, the average gestational age at diagnosis was 27 weeks, while the cyst size most often ranged from 20 to 50 mm. [69] In addition, structural malformations were observed and karyotype abnormalities were recorded, most often Trisomy 18 or Trisomy 13.

Omphalocele may be associated with umbilical cord cysts. [70] As expected, when associated with omphalocele, there is a high rate of karyotype abnormalities, particularly Trisomy 18.

Other true cysts such as omphalomesenteric duct cyst are rare, but may be associated with omphalocele. [71] Neonatal complications related to small bowel prolapse through an omphalomesenteric duct cyst are possible. Intestinal polyps are derivatives of the omphalomesenteric duct and may present as a solid tumor of the umbilical cord. The detection of these lesions allows for early neonatal surgical intervention.
Allantoic duct cysts and a patent urachus may coexsist, and megacystis may complicate this arrangement.[72] MRI should be considered for diagnostic purposes when an allantoic cyst is suspected. In the absence of malformations, allantoic cysts need close surveillance since their central position within the cord may be associated with umbilical blood flow compromise. Other potential fetal threats include umbilical cord vascular lesions, such as hematomas.
Solid Cysts

An angiomyxoma is a hemangioma. It represents a solid tumor with its origin from umbilical vessels. The differential diagnosis includes umbilical cord teratoma, umbilical cord polyp, other umbilical cord cysts, and omphalocele. [73] An angiomyxoma, while relatively large in size (8 cm), may be associated with optimal outcome.[74]
Umbilical Cord Cysts: Imaging Considerations
Umbilical cord cysts are classified as true cysts or pseudocysts. They may range in size from 4 mm to 60 mm. Despite this classification, it is difficult to distinguish between true cysts and pseudocysts on ultrasound imaging. [75] Most often true cysts are near the cord insertion site, while pseudocysts are more common.
First trimester umbilical cord cysts are most often detected between 8 and 9 weeks gestation, and their significance is controversial. Structural anomalies and chromosomal abnormalities are detected in up to 25% of high risk patients. [76] Single umbilical cord cysts compared to multiple umbilical cord cysts detected in the first trimester tend to have better outcomes. [77]
In a review of umbilical cord cysts in the second and third trimesters of pregnancy, the correlation between cyst appearance and prognosis is not consistent, but there is a high association among umbilical cord cysts, omphalocele, and patent urachus. [78] Second and third trimester umbilical cord cysts are also associated with aneuploidy, including Trisomy 13 and 18. Some authors recommend karyotype with umbilical cord cysts, especially in the presence of structural malformations. [79]
Allantoic cysts are the result of leakage of urine from the bladder through a patent urachus. They are located at the cord insertion site and can result in megacystis and compression of the umbilical cord at the site of insertion. Fetal death may follow. [80] Omphalo-mesenteric cysts are rare and few have been reported.
Summary
1. Cysts are thin-walled, anechoic, single or multiple. They range in size from 4 mm to 60 mm.
2. Look for umbilical cord cysts in the first trimester.
3. If present, consider genetic screen and genetic ultrasound in the second trimester.
4. Consider karyotype if there are multiple cysts and/or structural abnormalities.
5. Single small cysts in the first trimester tend to regress with gestational age.
6. Single small cysts in the first trimester have a better prognosis than multiple cysts.
7. True cysts are not distinguishable from pseudocysts on ultrasound imaging.
8. Note cysts location (abdominal cord insertion site, mid-cord, or near the placenta).
9. If the cyst is single and near abdominal cord insertion, assess the fetal bladder and anechoic areas within the fetal abdomen consistent with patent urachus.
Umbilical Cord Cysts: Images


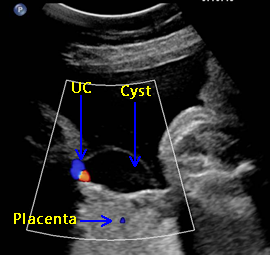
Above. 2-D gray scale transverse view of the UC (umbilical cord). Note thin-walled anechoic cyst. This unilateral cyst is most likely a pseudocyst (filled with Wharton’s jelly with cyst lining the cuboidal epithelium) although it is not possible to distinguish between true cysts and pseudocysts with ultrasound imaging.


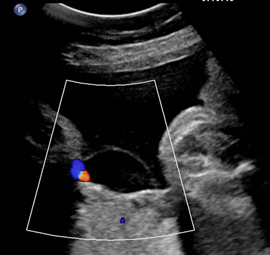
Above. Transverse of view of the UC (umbilical cord) with color Doppler. Note the umbilical cord vessels and the thin-walled anechoic cyst.
Above. Color Doppler image demonstrating the UC (umbilical cord) near the placental insertion site. Note the relatively large anechoic cyst.


Above. An angiomyxoma is a hemangioma of the umbilical cord. Note the more solid areas near the umbilical cord and the associated multiple pseudocysts.


Above. Note the anechoic allantoic cyst at the abdominal umbilical cord insertion site. The UA (umbilical artery) is noted separately superior to the cyst.


Above. Same patient as above. Oblique 2-D gray scale view. Note UC (umbilical cord) and CI (cord insertion) site. The anechoic urachus is visualized near the cord insertion.


Above. Same patient as above. Note the CI (cord insertion) and the UA (umbilical artery), which is coursing around the BL (bladder). The urachus extends from the fetal bladder towards the cord insertion site and the allantoic cyst. These structures are filled with fetal urine.
Umbilical Cord Cysts: Video
Above. Mid-trimester scan. Video courtesy of Dr. Firoz Bhuvar; World Ultrasound, Color Doppler, and Echo Society.
“Umbilical cord cyst possibilities include pseudocyst or true cyst – allantoic or omphalomesenteric duct cyst.” The cyst wall (above) is thickened and may have “epithelial cell lining plus the cyst is centrally located” and there is “widening of the umbilical arteries.” The cyst is near the fetal cord insertion site. Given these findings, allantoic cyst is most likely, but final diagnosis awaits follow-up and histology following birth. Commentary provided by Michelle Proctor, MD.
Top of Page
References-End
Moore KL and Persaud TVN. The Developing Human-Clinically Oriented Embryology. Fifth Edition WB Saunders Company. Philadelphia. 1993. Moore KL and Persaud TVN. The Developing Human-Clinically Oriented Embryology. Fifth Edition WB Saunders Company. Philadelphia. 1993. Bonilla-Musoles F, Machado LE, Osborne NG, Raga F, Bonilla F, Puig MJ, Machado F. Morphological assessment of the umbilical cord with three-dimensional ultrasonography. The Ultrasound Review of Obstetrics and Gynecology. 2002 Jan;2(1):17-42. -
Abstract: PMID: 11778994 -
Abstract: PMID: 16076617 -
Abstract: PMID: 17302517 -
Abstract: PMID: 11936081 -
Abstract: PMID: 15328432 -
Abstract: PMID: 17960667 -
Abstract: PMID: 17042061 -
Abstract: PMID: 12151155 -
Abstract: PMID: 11178630 Ultrasonography in pregnancy. ACOG Practice Bulletin: Number 101, February 2009. American College of Radiology. ACR practice guideline for the performance of obstetrical ultrasound. In: ACR practice guideline and technical standards, 2007. Reston (VA);2007.p.1025-1033. Moore KL and Persaud, TVN. Umbilical Cord: SUA. In: The Developing Human-Clinically Oriented Embryology. Fifth Edition. WB Saunders Company Philadelphia. 1993. -
Abstract: PMID: 16260215 Tuncay N, Ercan Y, Aylar P, Pinarzcan K, Aydan B, Rifat G. Antenatal diagnosis of umbilical artery fusion: a case report and review of the literature. Perinatal Journal. 2006;14(4):199-201. -
Abstract: PMID: 11392591 -
Abstract: PMID: 18297613 -
Abstract: PMID: 16232174 -
Abstract: PMID: 14726810 -
Abstract: PMID: 12575017 -
Abstract: PMID: 17999408 -
Abstract: PMID: 12648433 -
Abstract: PMID: 17994564 -
Abstract: PMID: 17538487 -
Abstract: PMID: 17286313 -
Abstract: PMID: 15940081 -
Abstract: PMID: 14689527 -
Abstract: PMID: 14689527 -
Abstract: PMID: 15863549 -
Abstract: PMID: 18548398 Murat M, et al. Evaluation of cases with single umbilical artery. Umbilical Cord: SUA. In: Perinatal Journal. 2006;14(3):117-121. -
Abstract: PMID: 17436317 -
Abstract: PMID: 17652931 -
Abstract: PMID: 16764013 Ahmadi F, Vosough Taghi Dizaj A, Irani S. Prenatal diagnosis of fetal umbilical vein varix in an intracytoplasmic sperm injection conception: a case report. Iran. J. Radiol. 2007;4(2):117-119. -
Abstract: PMID: 16389043 -
Abstract: PMID: 15042382 -
Abstract: PMID: 16498367 -
Abstract: PMID: 15685644 -
Abstract: PMID: 11211133 -
Abstract: PMID: 15305101 -
Abstract: PMID: 11169296 Cruise K, Rouse G. Klippel-Trenaunay-Weber Syndrome complicated by extra-fetal umbilical vein varix. Journal of Diagnostic Medical Sonography. 2002;18(5): 317-320. -
Abstract: PMID: 10864059 -
Abstract: PMID: 16749967 -
Abstract: PMID: 11169334 -
Abstract: PMID: 15229845 -
Abstract: PMID: 6846437 -
Abstract: PMID: 16858739 -
Abstract: PMID: 8839406 -
Abstract: PMID: 10395130 Shamas AG, Kambhapati L, Abu-Ghazza O, Dabbagh Z, Abdul-kadirbi R. Prenatal diagnosis of velamentous cord insertion and vasa praevia using ultrasound and magnetic resonance imaging: a case report. Ultrasound. 2008;16(1):15-17. -
Abstract: PMID: 15498919 -
Abstract: PMID: 10725492 -
Abstract: PMID: 17592490 Hasegawa Jun’ichi, Ichizuka Kiyotake, Matsuoka Ryu, Otsuki Katsufumi, Sekizawa Akihiko, Okai Takashi. A case report of velamentous cord insertion with abruption of the placenta. Journal of Japan Society of Perinatal and Neonatal Medicine. 2004;40(1):95-98. -
Abstract: PMID: 16858739 -
Abstract: PMID: 16479618 -
Abstract: PMID: 15907847 -
Abstract: PMID: 12808673 -
Abstract: PMID: 16870889 -
Abstract: PMID: 16479618 -
Abstract: PMID: 10725492 -
Abstract: PMID: 12666213 -
Abstract: PMID: 9052602 -
Abstract: PMID: 20131340 -
Abstract: PMID: 10074983 -
Abstract: PMID: 20131340 -
Abstract: PMID: 12666212 -
Abstract: PMID: 20103802 -
Abstract: PMID: 24591896 -
Abstract: PMID: 9542748 -
Abstract: PMID: 20131340 -
Abstract: PMID: 12666212 -
Abstract: PMID: 12666213 -
Abstract: PMID: 20131340 -
Abstract: PMID: 19848330 -
Abstract: PMID: 20103802
1
2
3
13
14
15
17
33
37
45
54
58