 Search
Search
Normal Umbilical Cord Development
Page Links: Umbilical Cord Development, Umbilical Cord Blood Flow, Imaging Considerations, Images, Summary, Video, References

The critical embryological times are at 24 to 25 days, the beginning of the 6th week, and during the 10th week. At 24 to 25 days, the abdominal wall forms and the yolk sac and its connections to the midgut are established. The intestines project into the cord at the beginning of the 6th week and during the 10th week, the intestines return to the abdomen. [Moore KL and Persaud TVN. The Developing Human-Clinically Oriented Embryology. Fifth Edition WB Saunders Company. Philadelphia. 1993.]


Graphic by John D’Agostino (modified).
Above. Left. The umbilical cord (UC) is derived from the stalk of the yolk sac, while the yolk stalk fuses with the omphalomesenteric duct (OMD). The out pouching of bladder (Bl) forms the urachus (U). The urachal extension into the cord forms the allantois (Al). The allantoic vessels become the umbilical vessels.
Above. Right. To the right is a transverse view of the fetal abdomen at about 9 weeks showing projection of the midgut into the umbilical cord insertion site.
Above. From the 6th through the 9th week, the developing intestines project into the umbilical cord insertion site.1
Umbilical Cord Blood Flow


Above. The normal umbilical cord has 2 umbilical arteries (UA) and 1 umbilical vein (UV). The umbilical arteries are branches of the fetal internal iliac arteries and bring deoxygenated blood from the fetus to the placenta. Each artery courses around the fetal bladder and enters the umbilical cord at the abdominal CI (cord insertion site). The umbilical vein brings oxygenated blood from the placenta to the fetus and enters the fetal liver at the abdominal cord insertion site. About 50% of the umbilical venous blood is shunted through the ductus venosus to the inferior vena cava before entering the right atrium.

Above. Longitudinal gray scale view. The umbilical vein (UV) enters the abdominal cord insertion site. The LPV (left portal vein) receives well-oxygenated blood from the umbilical vein and continues to the DV (ductus venosus) and then to the IVC (inferior vena cava) and right atrium.
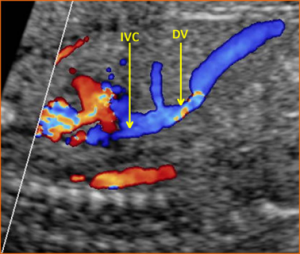
Above. Longitudinal view. Color Doppler. The umbilical vein enters the fetal liver. Note the flow through the ductus venosus (DV) and inferior vena cava (IVC) with well-oxygenated blood entering the right atrium.
Imaging Considerations

All aspects of umbilical cord development are complete by 10 to 11 weeks gestation. [Moore KL and Persaud TVN. The Developing Human-Clinically Oriented Embryology. Fifth Edition WB Saunders Company. Philadelphia. 1993.] The normal umbilical cord is shown with its placental insertion site and is covered by a glistening layer of amnion. The average length is 55 cm. and it may be spiraled or helical. [Bonilla-Musoles F, Machado LE, Osborne NG, Raga F, Bonilla F, Puig MJ, Machado F. Morphological assessment of the umbilical cord with three-dimensional ultrasonography. The Ultrasound Review of Obstetrics and Gynecology. 2002 Jan; 2(1): 17-42.]
Two dimensional images of umbilical cord should include the following:
- Gray scale transverse views
- Placental cord insertion site
- Abdominal cord insertion site
- Color Doppler transverse views
- Color Doppler arterial flow around fetal bladder
Images

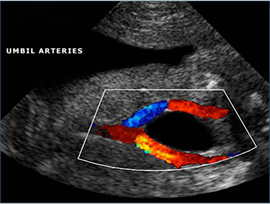
Above. Color Doppler image. Normal umbilical artery flow with 2 umbilical arteries coursing around the fetal bladder.
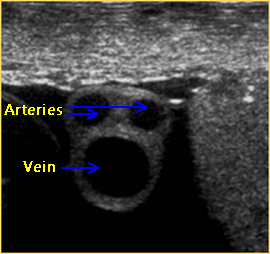

Above. 2-D gray scale and transverse view of the umbilical cord demonstrating 2 arteries of equivalent size and the larger umbilical vein.


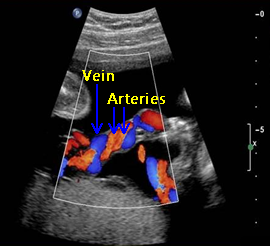
Above. Color Doppler image. Transverse view of normal umbilical cord demonstrating 2 arteries and 1 vein.
Above. Color Doppler image. Longitudinal view demonstrating 2 arteries and 1 vein.
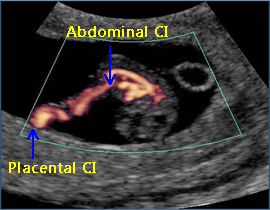

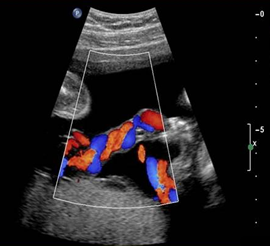
Above. Color power Doppler demonstrating both the placental cord insertion site and the abdominal cord insertion site. The umbilical cord (UC) diameter increases in size from 8 to 15 weeks. The UC diameter correlates with1 gestational age (GA), crown rump length (CRL), and biparietal diameter (BPD). By the end of the first trimester, there is normal blood flow in the mid-gut area.


Above. 2-D gray scale demonstrating abdominal cord insertion site. At 18 to 23 weeks, the umbilical cord diameter measured at the insertion into the fetal abdominal wall correlates with2 gestational age (GA), and estimated fetal weight (EFW).


Above. 2-D gray scale. Transverse view of the fetal abdomen. Note UC (umbilical cord) insertion at the fetal abdomen with a view of the UV (umbilical vein) with its entry into the fetal liver. At 24-39 weeks, the umbilical cord cross sectional area measured at insertion into fetal abdominal wall correlates with3 gestational age (GA).


Above. 2-D gray scale. Transverse view of the fetal abdomen. Again, note umbilical cord insertion into the fetal abdomen. The UA (umbilical artery) and the UV (umbilical vein) are noted.


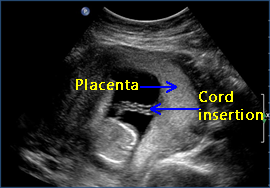
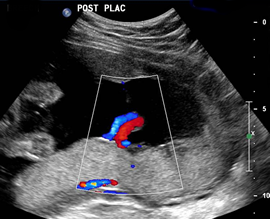
Above. 2-D gray scale. Normal umbilical cord insertion into the placenta. The placenta is posterior and the vascular pattern within the placenta suggests a 3 vessel cord.
An umbilical cord diameter of less than the 5th percentile for gestational age correlates with spontaneous miscarriage and preeclampsia. Umbilical cord diameter and umbilical cord thickness at 14-23 weeks4 and 18 to 23 weeks5 respectively correlate with the presence of fetal aneuploidy.
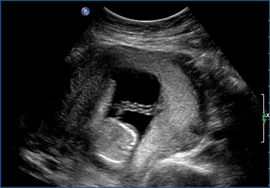
Above. 2-D gray scale demonstrating normal umbilical cord insertion into a laterally implanted placenta.

Above. Color Doppler image. Note central cord insertion site into the placenta. Umbilical cord with large cross sectional area at > 34 weeks correlates with the presence of fetal macrosomia at > 4000 grams and > 4500 grams.6 In that study, the correlation with macrosomia was best when an umbilical cord area exceed 250 mm2 and the abdominal circumference was > 9th percentile for gestational age. The umbilical artery discordant size does not affect outcome with the average luminal size variation being 13.1%.7


Above. Color Doppler image. Note the anterior placenta with central cord insertion. The umbilical vein cross sectional area at > 20 weeks and reduced Wharton’s jelly also correlates with perinatal death and NICU admissions.8
Excessively long umbilical cords occur and are associated with a variety of adverse perinatal events.9 Seventy centimeters is usually considered excessive umbilical cord length.
Essential ultrasound views for every ultrasound exam include a 3-vessel view and cord insertion into the fetal abdomen. [Ultrasonography in pregnancy. ACOG Practice Bulletin: Number 101, February 2009.] [American College of Radiology. ACR practice guideline for the performance of obstetrical ultrasound. In: ACR practice guideline and technical standards, 2007. Reston (VA); 2007. pp 1025-1033.]
Three vessel confirmation can be obtained by demonstrating 2 umbilical arteries around the fetal bladder or a transverse view of the cord in 2 D or color Doppler.
Demonstrating a normal cord insertion into the anterior abdomen is the other essential view, and can be performed with the use of gray scale or color Doppler imaging.
Summary
Normal Umbilical Cord Summary
1. Essential elements for a standard ultrasound examination include demonstration of: A). the number of fetal vessels and B). the cord insertion into the fetal abdomen.
2. The normal umbilical cord is coiled or helical, covered by a glistening layer of amnion and Wharton’s jelly, and measures approximately 50 cm. in length.
3. The first trimester cord increases in size from 8 to 15 weeks and the umbilical cord diameter correlates with gestational age, crown rump length, and biparietal diameter.
4. At 18 to 23 weeks, the umbilical cord diameter correlates with gestational age and estimated fetal weight.
5. At 24-39 weeks, the umbilical cord cross sectional area measured at insertion into fetal abdominal wall correlates with gestational age.
6. Areas of investigation which may hold promise for clinical care include:
a). Umbilical cord diameter which correlates with spontaneous miscarriage, preeclampsia, and aneuploidy.
b). Umbilical cord cross sectional area which correlates with fetal macrosomia at > 4000 grams and > 4500 grams.
Videos
Above. 2-D gray scale. 14 weeks gestation. Central cord insertion into anterior placenta.
Above. Color Doppler video. Central cord insertion into posterior placenta.