 Search
Search
The following topics are covered in this course:
Normal Kidney
Pyelectasis
Uretero-pelvic Junction Obstruction
Normal Kidney
Page Links: Transverse Views Kidney, Coronal Views Kidney, Renal Arteries, Fetal Bladder, References
The kidneys can be visualized as early as 9 to 12 weeks gestation, especially with transvaginal ultrasound. Urine production starts by 10 weeks gestation, [1] but is not a significant contributor to amniotic fluid volume until 15 weeks or greater. At 18 to 20 weeks, the kidneys are slightly hyperechoic compared to the surrounding tissues including the fetal bowel. [2] The renal pelvis is seen as an echo-free area and the ureters are not normally visualized. As the pregnancy advances, the renal echogenicity increases, and during the last trimester, the kidneys are surrounded by peri-renal fat while the pyramids are echogenic. The bladder is identified as an echo-free structure in the central pelvis and should always be observed during the second and third trimesters.
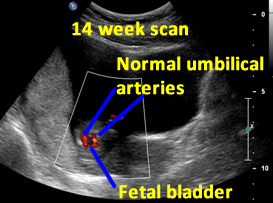

Above. Patient A. 14 weeks gestation. The fetal bladder and the umbilical arteries around the bladder are identified.
Transverse View of the Kidneys


Above. Patient B. 20 weeks gestation. Classic transverse view with spine dorsal position and kidneys well defined. The renal pelvis is 2 mm in the anterior posterior (AP) diameter, which is within normal limits. Cursor placement is inner to inner as demonstrated.


Above. Patient C. 18.2 weeks gestation. Transverse view. Spine is now lateral and inferior to the classic dorsal position, but the right kidney is well imaged in this position.
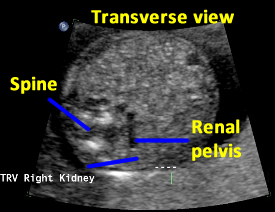

Above. Patient C. 18.2 weeks gestation. Transverse view. Spine is again lateral and inferior to the classic dorsal position. While the kidney is inferior to the spine, visualization is acceptable.


Above. Patient D. Transverse view. Mid-trimester. Renal outline appears circular and the renal pelvis is well defined.
Coronal View of the Kidneys
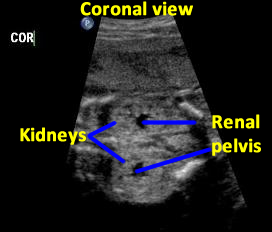

Above. Patient C. 18.2 weeks gestation. Coronal view. Both kidneys can be imaged and measured in this plane. The renal pelvis is seen, is symmetrical, and measures within normal limits in the AP diameter.

Above. Patient C. 18.2 weeks gestation. Coronal view. Each individual kidney can also be measured in this plane.


Above. Patient C. 18.2 weeks gestation. Coronal view. Again, each individual kidney can also be measured in this plane.


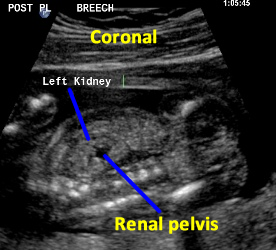
Above. Mid-trimester. Longitudinal view. The kidney is well outlined and the normal renal pelvis is visualized.
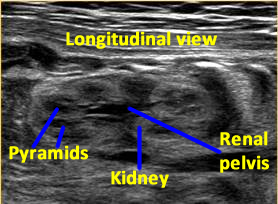

Above. 33 weeks gestation. Renal pyramids are echopenic. Peri-renal fat outlines the kidney and the renal pelvis is normal.
Renal Arteries
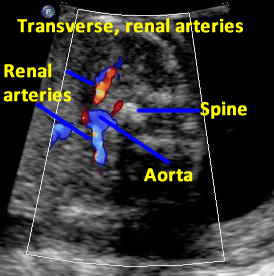

Above. Patient D. 20 weeks gestation. Transverse to oblique view. Color Doppler of the renal arteries.


Above. Patient E. 20 weeks gestation. Coronal view. Color power Doppler of the renal arteries.
Fetal Bladder


Above. Patient F. 20.2 weeks gestation. Coronal view with the fetal bladder in relation to the rest of the intra-abdominal organs.
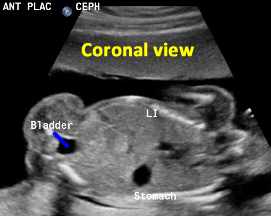

Above. Patient G. 19 weeks gestation. Again, Coronal view with the fetal bladder in relation to the rest of the intra-abdominal organs.
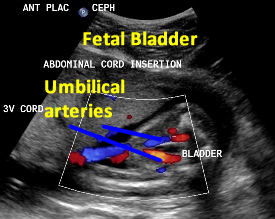

Above. Patient F. 20.2 weeks gestation. Umbilical arteries entering into the umbilical cord after coursing their normal anatomic position outlining the fetal bladder.
Pyelectasis
Top of Page
Page Links: Definition, Incidence and General Characteristics, Outcome, Postnatal Evaluation, Isolated Pyelectasis and Trisomy 21, Down Syndrome, References
Definition

Pyelectasis is dilatation of the renal pelvis of the kidney. A value of ≤ 4mm. in the anterior-posterior (AP) diameter of a transverse scan of the fetal kidney is considered a normal value irrespective of gestational age and a value of between 5 mm. to 10 mm. is considered borderline depending upon gestational age. Numerous cutoff values are reported in the literature. The most quoted, classic and recommended cutoffs for postnatal follow up studies are an AP pelvic diameter of ≥ 4 mm. at < 33 weeks and/or ≥ 7 mm. after 33 weeks.1
There are two areas of clinical interest:
1. dilatation of the renal pelvis for prediction of neonatal renal abnormality and,
2. dilatation of the renal pelvis as a soft marker predictor for Trisomy 21 (Down syndrome).
Incidence and General Characteristics

The incidence of pyelectasis is variously reported as between 1.7%2 and 4.5%.3 Renal pelvis AP dilatation is correlated with advancing gestational age4, and males are more commonly affected in both the normal and abnormal groups.5 There may be a genetic predisposition since occurrence is more common in consecutive pregnancies of affected fetuses.6
Outcome

The data on prognosis and outcome for pyelectasis is difficult to quantify due to the varied AP diameter cutoff levels and gestational ages, which are variously reported among relevant studies, but adverse neonatal outcome is possible. In general the second trimester ultrasound is the screen for pyelectasis but a 3rd trimester ultrasound better predicts neonates who require surgery for hydronephrosis.7 Over half of the children with hydronephrosis had prenatal ultrasound findings, 61% of which were pyelectasis. [Czarniak P, Zurowska A, Szcześniak P, Drozyńska-Duklas M, Maternik M, Gołebiewski A, Komasara L, Preis K, et al. Preliminary results of a program for the early management of children with congenital hydronephrosis. Pol Merkur Lekarski. 2009 Apr;26(154):322-4.]8
Prognosis for pyelectasis is dependent upon 3 factors9:
1. the magnitude of the dilatation,
2. caliceal dilatation and
3. the presence of hydroureter.
Fetuses with pyelectasis plus an additional ultrasound feature suggestive of urinary anomaly, such as enlarged bladder or kidney and/or ureteral or caliceal abnormality, required significantly more pediatric urology care after birth.10
Among 778 neonates referred for renal evaluation, 92% were referred on the basis of pyelectasis.11 In those studies, 76% of the neonatal scans were normal and 13% were associated with obstructive uropathy. Pyelectasis was found to be a poor predictor of vesicoureteral reflux (VUR).

The best outcome for pyelectasis is a value of <7.0 mm. obtained at ≥ 33 weeks in patients scanned between 18 and 30 weeks.12
Mild to moderate pyelectasis is associated with urinary abnormalities in up to 39% of infants.13 In fetuses who had 2 scans demonstrating renal pelvis dilatation before birth, those with no change demonstrated worsening after birth in 18.6% and those with worsening of the dilatation on consecutive scans demonstrated worsening after birth in 23.9%.14 Further, fetuses demonstrating ≥ 8 mm. AP diameter of the renal pelvis after 28 weeks showed renal pathology after birth in 2 of 3 cases.15
When the AP diameter of the renal pelvis is ≥ 4mm. during the 2nd trimester the neonatal uropathy rate is 12% but if the renal pelvis is ≥ 7 mm. but < 15 mm. during the 3rd trimester the neonatal uropathy rate is 39%.3
Renal pelvis progression to > 10 mm. occurs in 10.9% of cases when the renal pelvis AP diameter is > 4 mm. at < 32 weeks or > 7 mm. at ≥ 32 weeks.16
When hydronephrosis occurs (AP diameter of > 10 mm.) at 20 to 30 weeks gestation or > 16 mm. at > 33 weeks gestation, renal function is affected.17
In summary, a second fetal renal scan or a 3rd trimester scan with a cutoff of ≥ 10 mm. will detect most cases of neonatal renal pathology while a ≥ 8 mm. value has low specificity but will include most cases of pathology.18
Postnatal Evaluation

Prenatal ultrasound of the urinary tract has the highest false positive rate among malformations and approximately 20% of abnormal fetal urinary tract observations noted before birth are not present after birth19and prenatal ultrasound is less sensitive than the postnatal scan in defining obstructive uropathy. If the neonatal scan demonstrates an AP diameter of the renal pelvis of < 10 mm., this is reassuring since virtually all patients normalize within 1 year.20
The most specific time to conduct a neonatal ultrasound is 6 weeks after birth rather than 6 days after birth since non-obstructed kidneys demonstrate no change during this interval while obstructed kidneys show a mean increase in diameter during this interval.
In cases of pyelectasis if the neonatal ultrasound is normal, no further evaluation is needed. If the neonatal ultrasound shows isolated pyelectasis of < 10 mm. or < 15 mm. in uninfected cases of vesicoureteral reflux, voiding cystourethrogram can be delayed since cases within these parameters spontaneously resolve. [Masson P, De Luca G, Tapia N, Le Pommelet C, Es Sathi A, Touati K, Tizeggaghine A, Quetin P. Postnatal investigation and outcome of isolated fetal renal pelvis dilatation. Arch Pediatr. 2009 Aug;16(8):1103-10.]21
Isolated Pyelectasis and Trisomy 21, Down Syndrome
Markers for fetal aneuploidy include: any structural malformation, nuchal fold thickening, short long bones (humerus and femur), echogenic heart, hyperechoic bowel and pyelectasis; there are no apparent gender differences among sonographic markers for Down syndrome noted during the second trimester.22

Among 44 fetuses with Down syndrome, 25% had pyelectasis23 but studies which evaluate the significance of soft markers for fetal aneuploidy are varied and often contradictory.24 However, a recent study of over 60,000 scans reported that a > 4 mm. dilatation of the renal pelvis was associated with fetal aneuploidy, especially trisomy 21, and that the odds ratio for trisomy 21 with this criteria was 2.91 (CI=1.48-5.71).2 In summary, the sensitivity for Down syndrome detection is increased to 80.5% with a false positive rate of 12.4% in the presence of any marker, while pyelectasis as an isolated finding has a relatively low likelihood ratio.25
Top of Page
Imaging Considerations (Pyelectasis)
Page Links: Imaging Considerations, Measurements, References
The overall sonographers’ tasks are as follows:
Sonographer Tasks:
- Measure renal pelvis through transverse view of the kidney.
- Take measurement when fetal bladder is empty, if possible.
- Measure largest anterior posterior diameter of the renal pelvis in mm.
- Obtain longitudinal view of fetal kidney.
- Observe for presence of calectasis.
- Assess contralateral kidney
- Measure longitudinal diameter of renal pelvis.
- Measure longitudinal diameter of the fetal kidney.
- Use color Doppler to assess for renal artery blood flow to each kidney.
The values for renal pelvis dilatation are taken from a number of studies. 1–5 Renal pelvis measurements change with gestational age. In general, ≥ 7 mm. is considered abnormal irrespective of gestational age. At <33 weeks, ≥ 5 mm. is generally considered the cutoff and a repeat measurement at ≥ 33 weeks is recommended. Neonatal follow up is recommended if the repeat measurement is ≥ 7 mm.
Measurements
Initial studies showed no relationship between maternal hydration and the degree of pyelectasis 6 , but follow up studies were not always confirmatory. In addition, the size of the renal pelvis measurement over a 2 hour period is variable 7 and the size also varies with bladder filling. 8 Fetal bladder sagittal length can help calculate a normal versus an enlarged fetal bladder. 9 In light of these findings, AP measurements of the renal pelvis should be conducted as often as possible when the fetal bladder is empty.


Above. Patient A. Transverse view of kidneys with mild bilateral renal pelvis dilatation.
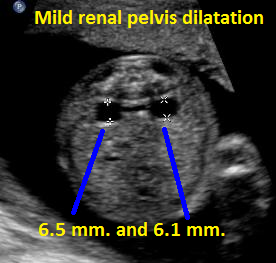

Above. Patient B. Transverse view of kidneys with mild bilateral renal pelvis dilatation.
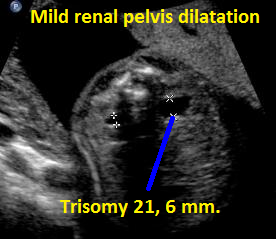

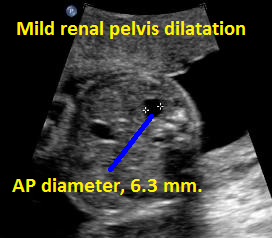
Above. Patient C. Transverse view. Mild renal pelvis dilatation; fetus with known Trisomy 21.


Above. Patient C. Sagittal view. Mild renal pelvis dilatation; fetus with known Trisomy 21.

Above. Patient D. Borderline mild unilateral renal pelvis dilatation.


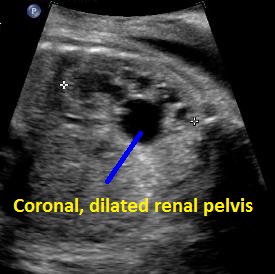
Above. Patient D. Coronal view. Borderline unilateral renal pelvis dilatation.


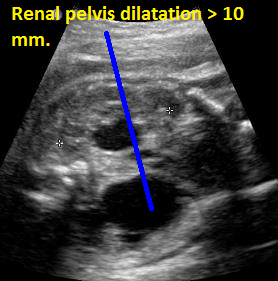
Above. Patient E. Transverse to oblique view with AP diameter of renal pelvis > 10 mm, designating a label of “hydronephrosis.”


Above. Patient E. Coronal view demonstrating dilatation of the renal pelvis and the presence of 2 kidneys by Color flow Doppler.


Above. Patient F. Transverse view of kidneys. Unilateral increase in dilatation of the renal pelvis which defines hydronephrosis (AP diameter of > 10 mm). Further assessment requires evaluation of pelvic, ureteral, or bladder obstruction.

Above. Patient F. Coronal view. Unilateral increase in dilatation of the renal pelvis which defines hydronephrosis (AP diameter of > 10 mm).
Above. Pyelectasis.
Above. Pyelectasis.
Uretero-pelvic Junction Obstruction
Top of Page
Page Links: Definition, Measurements and Critical Cutoff Values, Incidence, Pathophysiology, Diagnosis, Biomarkers, Management, Surgery, Mass Screening, References
Definition
Ureteropelvic junction (UPJ) obstruction: obstruction of the urinary tract where the renal pelvis meets the ureter. This excludes dilatation of the ureter and/or bladder.
Measurements and Critical Cutoff Values

Measurement is taken in the anterior-posterior (AP) diameter of a transverse scan of the fetal kidney.
Normal value irrespective of gestational age: ≤ 4 mm.
Borderline value: 5 mm. to 10 mm. depending upon gestational age.
Abnormal value: 4 mm. at < 33 weeks and/or ≥ 7 mm. after 33 weeks. [3]
Hydronephrosis: ≥ 10 mm. irrespective of gestational age.
Values above the critical cutoffs may signify either an obstructive or non-obstructive (reflux) etiology.
Incidence

The incidence of prenatally diagnosed abnormalities of the urinary tract is 0.5% of all pregnancies. [4] Hydronephrosis is one of the most commonly diagnosed congenital malformations, and UPJ obstruction is the leading cause of hydronephrosis, accounting for approximately 35% of cases. [5]

Some causes of hydronephrosis, in descending order of frequency, include UPJ obstruction, vesicoureteral reflux, ureterovesical junction (UVJ) obstruction, and posterior urethral valves (PUV). [6]
UPJ obstruction occurs more frequently in males; to female ratio is a 2.7; it is unilateral in about 61% and more frequent on the left side (68%). Bilateral obstruction occurs in approximately 39% of fetuses. [7] Prematurity and twinning are independently associated with UPJ obstruction. [8] Renal and urinary tract anomalies are more common in patients with Down syndrome (3.2%) compared to the overall population (0.7%). [9]
Pathophysiology

Antenatal urinary tract obstruction affects growth, maturation, and development of the kidneys by causing nephron reduction, atrophy of the tubules, and progressive interstitial fibrosis, all of which lead to programmed cell death and loss of tubular epithelial cells. [10]

A potential pathophysiologic explanation for congenital UPJ obstruction is as follows [11]: defective smooth muscle and nerve maldevelopment at the level where the ureter joins the renal pelvis leads to a functional obstructive defect, which delays urine ejection from the renal pelvis into the upper ureter on the basis of a non-peristaltic segment. Initial dilatation is compliant and does not result in renal parenchymal pressure from intra-pelvic pressure. However, increased intra-pelvic pressure results in tubular stretch and injury. As a consequence, a number of inflammatory, cellular, and chemical changes occur. Tubular cell death results in tubular atrophy. A vascular constrictive element may be contributory. [12] In congenital UPJ obstruction, renal histology is modified and the process includes not only inflammation and cell death, but also renin-angiotensin system activation and fibrosis. [13] Renal biopsies in patients undergoing pyeloplasty for UPJ obstruction may suggest relatively well-maintained parenchyma with findings of parenchymal thinning and only limited tubulointerstitial injury. [14] A variety of renal parenchymal changes occur with UPJ obstruction, and these changes are not concordant with observations from conventional imaging. [15] The angiotensin type II receptor print (AGT R-2) accounts for a wide variety of congenital renal abnormalities, and this gene likely plays a role in the development of obstructive nephropathy. [16]
Diagnosis

Antenatal diagnosis of UPJ obstruction is suspected when critical measurements of the AP diameter of the renal pelvis are exceeded (> 4 mm. at < 33 weeks and/or ≥ 7 mm. after 33 weeks) [17] in the absence of ureteral or bladder dilatation. If the AP diameter value is ≥ 10 mm. under these circumstances, hydronephrosis is defined and UPJ obstruction can be specified as a cause of hydronephrosis.
Biomarkers

A key determinant in treatment after birth is determining whether UPJ obstruction is due to an obstructive or non-obstructive origin. Noninvasive biomarkers for UPJ obstruction may define the clinical outcome in advance of definitive clinical abnormalities. [18] Certain voided urinary markers differentiate children with UPJ obstruction needing a pyeloplasty versus those with non-obstructed kidneys, which can be managed conservatively. [19]

Urinary polypeptides may predict with a high degree of precision (94%) which patients with UPJ obstruction require surgical correction. [20] Other biomarkers have been identified in children with obstructive uropathy and include urinary heme oxygenase-1 (HO-1), which decreases significantly after surgical correction of the obstructive process. [21] Neutrophil gelatinase-associated lipocalin (NGAL) and β2-microglobulin (β2-M) show promise in defining obstructed versus non-obstructed kidneys [22], while good diagnostic accuracy is achieved by measuring urinary concentrations of monocyte chemotactic protein-1 (MCP-1). [23] Finally, urinary poly peptides in newborns with UPJ obstruction may also predict clinical outcomes. [24]
Management

The management of neonatal UPJ obstruction is controversial. [25] The finding of significant dilatation of the renal pelvis may be from an obstructive or non-obstructive origin, which is not always apparent. In patients with UPJ obstruction, differential renal function is usually normal at birth and does not often show signs of high-grade obstruction. When differential renal function is stable or improving, severe hydronephrosis resolves in more than 65% of cases. [26] Therefore, UPJ obstruction in newborns with normal renal function can be managed conservatively in most cases. [27]

In patients with moderate renal functional abnormality who undergo pyeloplasty, 83% show improved renal function while infants with severely reduced renal function do not benefit by pyeloplasty. [28] Again, those with normal renal function most often show spontaneous resolution of the hydronephrosis.
Conservative management includes serial observation and evaluation utilizing renal ultrasound, voiding cystourethrogram, and renal flow scans (RFS). [29] In addition, retrograde studies may sometimes be useful. [30]
Indications for surgery include low differential renal function (DRF), absence of tracer clearance from the renal pelvis, parental preference, and acute renal failure. Pyeloplasty is considered the treatment of choice when the split difference in renal function is less than 40% and/or when the pelvic diameter is greater than 35 mm at initial evaluation. [31] Under these circumstances, the overall operative success rate is reported at 97.9%. Prophylactic antibiotics should be given before six months of age in those infants suspected of severe obstruction. [32]

Postnatal diagnosis of UPJ obstruction may be different from prenatal diagnosis. Postnatal UPJ obstruction more frequently affects females in later life, and presenting symptoms are urinary infection and/or abdominal pain with ureteral kinking as the likely etiology. [33]
Surgery

Pyeloplasty is the standard surgical procedure for UPJ obstruction. However, renal impairment remains after pyeloplasty in patients with urterovesicle reflux and pre-existing renal dysplasia. [34]
Other technically feasible surgical approaches include robotic laparoscopic single site pyeloplasty. [35] A high success rate with low morbidity is achieved in infants undergoing robot-assisted laparoscopic pyeloplasty [36], and other short-term studies demonstrate this approach to be safe and effective. [37] The number of laparoscopically performed pyeloplasty procedures for UPJ obstruction is increasing. However, some studies suggest no significant decrease in hospital length of stay whereas costs do increase. [38]
Mass Screening

Mass screening of infants at two months of age for congenital anomalies of the kidney and urinary tract (CAKU T) yields a frequency of 0.96% for affected infants. [39] However, the number of patients requiring surgery (0.24%) does not justify mass screening.
Page Links: Sonographer Tasks, Normal Values, Ultrasound Findings: UPJ Obstruction, Follow-up
Sonographer Tasks (UPJ)
Measure renal pelvis through transverse view of the kidney.
Take the measurement when the fetal bladder is empty if possible.
Measure the largest anterior/posterior diameter of the renal pelvis in millimeters and record.
Obtain longitudinal view of fetal kidney.
Observe for the presence of caliectasis.
Measure the longitudinal diameter of the renal pelvis.
Measure the longitudinal diameter of the fetal kidney.
Use color Doppler to assess for renal artery blood flow to each kidney.
Perform amniotic fluid index.
In isolated UPJ obstruction with borderline AP diameter values of 5 mm. to 10 mm., only 1 follow-up is needed at 33 weeks or later.
Normal Values

- The most quoted, classic and recommended cutoffs for postnatal follow-up studies are an AP pelvic diameter of 5 mm or greater at < 33 weeks or ≥ 7 mm. at or after 33 weeks.
- Always repeat a value of 5 mm. at < 33 weeks. Repeat at or after 33 weeks.
- Hydronephrosis (abnormal) is defined as the AP diameter of the renal pelvis of ≥10 mm.
Ultrasound Findings: UPJ Obstruction

- Hydronephrosis is present if AP diameter is ≥ 10 mm.
- Distension of central renal pelvis
- More often unilateral but may be bilateral
- No ureteral dilatation
- No bladder dilation or bladder wall thickening
- Size of distension varies
- 35 mm. cutoff important as an indication for neonatal pyeloplasty
- Increased male to female ratio
- Caliectasis may be present
- If obstruction is severe, it may be associated with renal dysplasia (echogenicity and/or renal cysts)
- If obstruction is bilateral, the bladder may be small and amniotic fluid volume decreased
Follow-up
If 5 mm. or greater at < 33 weeks repeat measurement at or after 33 weeks.
If ≥ 7 mm. after or at 33 weeks, refer for the neonatal exam, evaluation, and follow-up.


Above. Patient A. 33 weeks gestation. The bilateral AP diameter of the renal pelvis is 10.0 mm or greater.


Above. Patient A. 33 weeks gestation. Renal pelvis dilatation with evidence of caliceal dilation, but no ureteral or bladder obstruction.

Above. Patient B. 28 weeks gestation. Bilateral renal pelvis dilation of > 10 mm with right side greater than left side.


Patient B. 28 weeks gestation. Same as above. Bilateral renal pelvis dilation of > 10 mm with right side greater than left side.
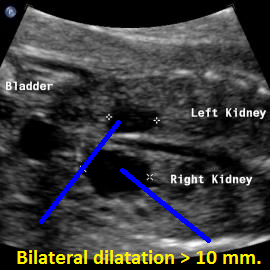

Above. Patient C. 20 weeks gestation. Bilateral renal pelvis dilation, but no evidence of ureteral, vesical, or outlet obstruction.


Above. Patient D. 28 weeks gestation. Massive renal pelvis dilatation is secondary to UPJ obstruction.


Above. Patient D. 28 weeks gestation. Massive renal pelvis dilatation is secondary to UPJ obstruction. Color flow Doppler demonstrates normal renal artery to the contralateral kidney.
Uretero-pelvic junction (UPJ) obstruction.
Above. UPJ Obstruction.
We are grateful to the generous contribution of images by Jane J.K. Burns, A.S., R.T., RDMS.
References: Pyelectasis Information
1. Corteville J., Gray D., Crane J. Congenital hydronephrosis: correlation of fetal ultrasonographic findings with infant outcome. Am J Obstet Gynecol 1991;165(2):384–8. [PubMed]
2.Carbone J., Tuuli M., Dicke J., et al. Revisiting the risk for aneuploidy in fetuses with isolated pyelectasis. Prenat Diagn 2011;31(6):566–70. [PubMed]
3. Ismaili K., Hall M., Donner C., et al. Results of systematic screening for minor degrees of fetal renal pelvis dilatation in an unselected population. Am J Obstet Gynecol 2003;188(1):242–6. [PubMed]
4.Odibo A., Marchiano D., Quinones J., et al. Mild pyelectasis: evaluating the relationship between gestational age and renal pelvic anterior-posterior diameter. Prenat Diagn 2003;23(10):824–7. [PubMed]
5.Wilson R., Lynch S., Lessoway V. Fetal pyelectasis: comparison of postnatal renal pathology with unilateral and bilateral pyelectasis. Prenat Diagn 1997;17(5):451–5. [PubMed]
6.Degani S., Leibovitz Z., Shapiro I., et al. Fetal pyelectasis in consecutive pregnancies: a possible genetic predisposition. Ultrasound Obstet Gynecol 1997;10(1):19–21. [PubMed]
7.Thornburg L., Pressman E., Chelamkuri S., et al. Third trimester ultrasound of fetal pyelectasis: predictor for postnatal surgery. J Pediatr Urol 2008;4(1):51–4. [PubMed]
8.Czarniak P., Zurowska A., Szcześniak P., et al. [Preliminary results of a program for the early management of children with congenital hydronephrosis]. Pol Merkur Lekarski 2009;26(154):322–4. [PubMed]
9.Broadley P., McHugo J., Morgan I., et al. The 4 year outcome following the demonstration of bilateral renal pelvic dilatation on pre-natal renal ultrasound. Br J Radiol 1999;72(855):265–70. [PubMed]
10.Maizels M., Wang E., Sabbagha R., et al. Late second trimester assessment of pyelectasis (SERP) to predict pediatric urological outcome is improved by checking additional features. J Matern Fetal Neonatal Med 2006;19(5):295–303. [PubMed]
11.Acton C., Pahuja M., Opie G., et al. A 5-year audit of 778 neonatal renal scans (Part 1): perplexing pyelectasis and suggested protocol for investigation. Australas Radiol 2003;47(4):349–53. [PubMed]
12.Odibo A., Raab E., Elovitz M., et al. Prenatal mild pyelectasis: evaluating the thresholds of renal pelvic diameter associated with normal postnatal renal function. J Ultrasound Med 2004;23(4):513–7. [PubMed]
13.Ismaili K., Avni F., Wissing K., et al. Long-term clinical outcome of infants with mild and moderate fetal pyelectasis: validation of neonatal ultrasound as a screening tool to detect significant nephrouropathies. J Pediatr 2004;144(6):759–65. [PubMed]
14.Signorelli M., Cerri V., Taddei F., et al. Prenatal diagnosis and management of mild fetal pyelectasis: implications for neonatal outcome and follow-up. Eur J Obstet Gynecol Reprod Biol 2005;118(2):154–9. [PubMed]
15.Adra A., Mejides A., Dennaoui M., et al. Fetal pyelectasis: is it always “physiologic”? Am J Obstet Gynecol 1995;173(4):1263–6. [PubMed]
16.Bobrowski R., Levin R., Lauria M., et al. In utero progression of isolated renal pelvis dilation. Am J Perinatol 1997;14(7):423–6. [PubMed]
17.Kim D., Mickelson J., Helfand B., et al. Fetal pyelectasis as predictor of decreased differential renal function. J Urol 2009;182(4 Suppl):1849–53. [PubMed]
18.Cohen-Overbeek T., Wijngaard-Boom P., Ursem N., et al. Mild renal pyelectasis in the second trimester: determination of cut-off levels for postnatal referral. Ultrasound Obstet Gynecol 2005;25(4):378–83. [PubMed]
19.Ebel K. Uroradiology in the fetus and newborn: diagnosis and follow-up of congenital obstruction of the urinary tract. Pediatr Radiol 1998;28(8):630–5. [PubMed]
20.Dremsek P., Gindl K., Voitl P., et al. Renal pyelectasis in fetuses and neonates: diagnostic value of renal pelvis diameter in pre- and postnatal sonographic screening. AJR Am J Roentgenol 1997;168(4):1017–9. [PubMed]
21.Masson P., De L., Tapia N., et al. [Postnatal investigation and outcome of isolated fetal renal pelvis dilatation]. Arch Pediatr 2009;16(8):1103–10. [PubMed]
22.Benacerraf B., Miller W., Nadel A., et al. Does gender have an impact on the sonographic detection of second-trimester fetuses with Down’s syndrome? Ultrasound Obstet Gynecol 1995;5(1):30–3. [PubMed]
23.Benacerraf B., Mandell J., Estroff J., et al. Fetal pyelectasis: a possible association with Down syndrome. Obstet Gynecol 1990;76(1):58–60. [PubMed]
24.Raniga S., Desai P., Parikh H. Ultrasonographic soft markers of aneuploidy in second trimester: are we lost? MedGenMed 2006;8(1):9. [PubMed]
25.Bromley B., Lieberman E., Shipp T., et al. The genetic sonogram: a method of risk assessment for Down syndrome in the second trimester. J Ultrasound Med 2002;21(10):1087-96; quiz 1097-8. [PubMed]
Top of Page
References: Pyelectasis Imagining Considerations
1.Corteville J., Gray D., Crane J. Congenital hydronephrosis: correlation of fetal ultrasonographic findings with infant outcome. Am J Obstet Gynecol 1991;165(2):384–8. [PubMed]
2.Bobrowski R., Levin R., Lauria M., et al. In utero progression of isolated renal pelvis dilation. Am J Perinatol 1997;14(7):423–6. [PubMed]
3.Ismaili K., Hall M., Donner C., et al. Results of systematic screening for minor degrees of fetal renal pelvis dilatation in an unselected population. Am J Obstet Gynecol 2003;188(1):242–6. [PubMed]
4. Odibo A., Marchiano D., Quinones J., et al. Mild pyelectasis: evaluating the relationship between gestational age and renal pelvic anterior-posterior diameter. Prenat Diagn 2003;23(10):824–7. [PubMed]
5.Odibo A., Raab E., Elovitz M., et al. Prenatal mild pyelectasis: evaluating the thresholds of renal pelvic diameter associated with normal postnatal renal function. J Ultrasound Med 2004;23(4):513–7. [PubMed]
6.Hoddick W., Filly R., Mahony B., et al. Minimal fetal renal pyelectasis. J Ultrasound Med 1985;4(2):85–9. [P
7.Persutte W., Hussey M., Chyu J., et al. Striking findings concerning the variability in the measurement of the fetal renal collecting system. Ultrasound Obstet Gynecol 2000;15(3):186–90. [PubMed]
8.Damen-Elias H., Stigter R., De J., et al. Variability in dilatation of the fetal renal pelvis during a bladder filling cycle. Ultrasound Obstet Gynecol 2004;24(7):750–5. [PubMed]
9.Maizels M., Alpert S., Houston J., et al. Fetal bladder sagittal length: a simple monitor to assess normal and enlarged fetal bladder size, and forecast clinical outcome. J Urol 2004;172(5 Pt 1):1995–9. [PubMed]
References Normal and UPJ Obstruction
Twining, P., Genitourinary malformations. In Diagnostic Imaging of Fetal Anomalies. Nyberg, DA, et al, eds. Lippincott, Williams, and Wilkins. 2003. PP: 604-05. Twining, P., Genitourinary malformations. In Diagnostic Imaging of Fetal Anomalies. Nyberg, DA, et al, eds. Lippincott, Williams, and Wilkins. 2003. PP: 604-05. -
Abstract: PMID: 1872344 -
Abstract: PMID: 10958739 -
Abstract: PMID: 22710694 -
Abstract: PMID: 22569439 -
Abstract: PMID: 19043723 -
Abstract: PMID: 18256845 -
Abstract: PMID: 19752083 -
Abstract: PMID: 15200251 -
Abstract: PMID: 22428472 -
Abstract: PMID: 15906780 -
Abstract: PMID: 20681980 -
Abstract: PMID: 18280506 -
Abstract: PMID: 16374434 -
Abstract: PMID: 16133060 -
Abstract: PMID: 1872344 -
Abstract: PMID: 17701042 -
Abstract: PMID: 17574624 -
Abstract: PMID: 16550189 -
Abstract: PMID: 22630328 -
Abstract: PMID: 22710694 -
Abstract: PMID: 22744767 -
Abstract: PMID: 18401166 -
Abstract: PMID: 12084278 -
Abstract: PMID: 18074126 -
Abstract: PMID: 15628642 -
Abstract: PMID: 15628642 -
Abstract: PMID: 19043723 -
Abstract: PMID: 19713154 -
Abstract: PMID: 18947602 -
Abstract: PMID: 17296419 -
Abstract: PMID: 15748309 -
Abstract: PMID: 11595845 -
Abstract: PMID: 22469392 -
Abstract: PMID: 22191495 -
Abstract: PMID: 19519760 -
Abstract: PMID: 18708209 -
Abstract: PMID: 22271367
1
2