 Search
Search
Normal Fetal Heart Ultrasound
Quiz: Introduction to the Fetal Heart Scan
Please note. To obtain the certificate, you must answer each quiz question, including the assessment questions. Your score is based upon the quiz questions only and not the assessment questions. A score of 70% or greater is necessary on the quiz questions to obtain the certificate, which is then made immediately available.
Page Links: Overview Aims, Fetal Heart Assessment: Gray Scale, 2-D Optimization, Screening Cardiac Exam, 11-13 Week Scan, Videos, Fetal Viabilty, Fetal Situs, Four Chamber View, Interventricular Septum, Atrial Views, Pulmonary Veins, Left Ventricular Outflow Tract (LVOT), Right Ventricular Outflow Tracts (RVOT), Three Vessel View (3 VV), Three Vessel Tracheal View (3VT), Aortic Arch, Ductal Arch, Color Doppler, References
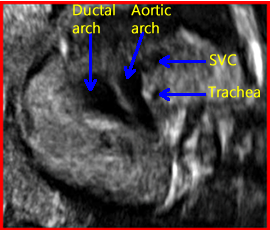
Above. 3 Vessel Tracheal View.
Overview Aims
The cardiac screening exam is one of the most important aspects of fetal assessment since congenital heart defects are a major cause of mortality and prenatal detection can improve outcomes. All major specialty organizations, including the American Institute for Ultrasound in Medicine (AIUM), recommend the four chamber, the left ventricular outflow tract (LVOT), and the right ventricular outflow tract (RVOT) views. (http://www.aium.org/resources/guidelines/obstetric.pdf). In addition, the transverse view of abdomen, the 3 vessel view (3VV), and the 3 vessel tracheal (3VT) view are recommended by the International Society of Ultrasound in Obstetrics and Gynecology (ISUOG). [1] The aim of the screening exam is to define normality and whether there is deviation from normality, requiring referral for fetal echocardiogram.
Fetal Heart Assessment: Gray Scale
To assess fetal cardiac anatomy, a disciplined approach is necessary and optimization of the 2-D equipment is necessary prior to application of color Doppler. This topic summarizes a stepwise approach to the ultrasound anatomy of the fetal heart.
2-D Optimization
Always follow the ALARA principle to use “as low as is reasonably achievable” to obtain satisfactory images. Use the highest frequency transducer, adjust the overall gain, correct depth, adjust sector width, decrease the compression or dynamic range, and adjust the focal zone. Use magnification or “zoom” to increase the frame rate and obtain cine loops and video clips to define anatomic details. The cardiac image should occupy approximately 1/3 to 1/2 of the ultrasound screen. Use a higher megahertz transducer prior to application of color Doppler.
Screening Cardiac Exam
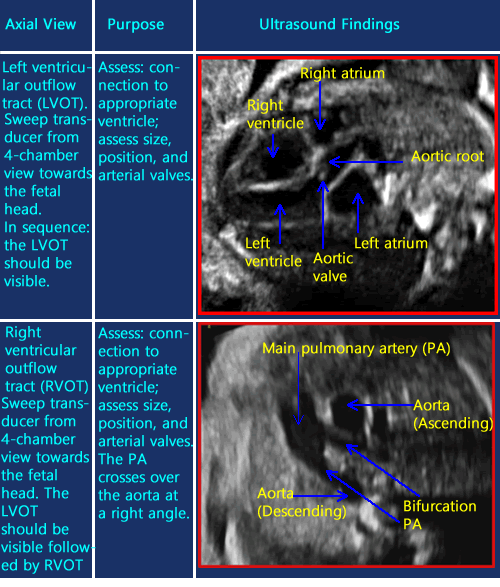
A summary of the key axial views of the heart will be presented as recommended by the ISUOG guidelines [2] followed by a more detailed description of fetal cardiac views and their significance.




Above images courtesy of Jill Beithon, RT, RDMS, RDCS, RVT.
11-13 Week Scan
“Prenatal detection of congenital heart defects at the 11-to-13 week scan using a simple color Doppler protocol including the 4-chamber and 3-vessel and trachea views” [3]:
In this prospective observational study performed at 11 to 13 weeks, among 1084 patients, 35 cases were confirmed to have a congenital heart defect. The most effective approach was color mapping of the 4 chamber and 3 vessel and trachea views. The ideal insonation beam was 45 degrees with the fetal spine at 6 o’clock. The transducer assessed ventricular inflows in color at the level of the 4 chamber view, the 3 vessel view and finally demonstrating the V sign at the level of the 3 vessel trachea view. Using this approach, a sensitivity of 88.5% and a specificity of 100% for the detection of CHDs at 11 to 13 weeks was achieved. In addition, the vascular patterns for many of the defects are presented.
Videos
Above. 4 chamber view. The LV (left ventricle) and ascending aorta are identified. The color Doppler indicates the aortic blood flow is, as expected, towards the transducer (red).
Above. LVOT (Left ventricular outflow tract). Note the LV (left ventricle) with the aorta and aortic valve are visible. This represents a key view (circled in red) for defining a VSD (ventricular septal defect).
Above. A short axis view demonstrating the RV (right ventricle), the MPA (main pulmonary artery), and the PV (pulmonary valve). In this view, the aorta is seen as the MPA crosses over it.
Above. Slightly oblique transverse view of the chest demonstrating the 3 vessel view in the appropriate order: the MPA (main pulmonary artery), the aorta, and the SVC (superior vena cava). The trachea is not well seen in this view.
Fetal Viability
Determine fetal viability by either M-mode or by direct visualization of fetal cardiac activity.
Fetal Situs
Situs solitus describes the normal position of fetal organs. (See also the chapter Fetal Situs). The fetal stomach is normally on the left side, the left atrium is nearest to the fetal spine, and the cardiac axis points to the left.
To determine fetus situs:
1. Define within the uterus the presentation of the fetus (generally, vertex or breech).
2. Determine whether the fetal spine is parallel or transverse to the maternal spine. In the sagittal view, if the fetal and maternal spine are parallel, the fetus is in longitudinal lie. When the fetal spine is perpendicular to the maternal spine, the fetus is in transverse lie.
3. Determine the position of the fetal left side.
The fetal left side will be as follows:
A. With respect to the maternal abdomen, the fetal left side is anterior and near to the ultrasound transducer.
B. With respect to the posterior uterine wall, the fetal left side is posterior and farthest from the transducer.
C. With respect to the right uterine wall, the fetal left side will be on the maternal right.
D. With respect to the left uterine wall, the fetal left side will be on the maternal left.
4. Obtain a transverse view of the abdomen and define the fetal stomach, which is positioned in the left side of the abdomen.
5. Obtain a 4 chamber view of the heart by obtaining a transverse view of the thorax. The left atrium and descending aorta are nearest to the spine and the cardiac axis points to the left.
6. Finally, ascertain if the stomach and heart are in their correct respective locations, i.e., the stomach is on the left side and the cardiac axis points to the left.
7. Place a transverse image of the fetal abdomen and heart side by side and validate that the left side of the fetal abdomen (stomach near to the spine) is concordant with the left side of the fetal heart (left atrium and descending aorta near to the spine, and cardiac axis points to the left). This is done by displaying a side by side comparison of a transverse view through the fetal stomach and a 4 chamber cardiac view.
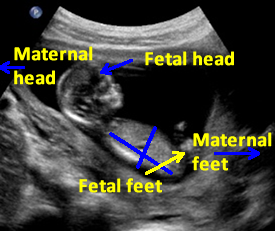

Above. The fetus is in breech presentation, the spine and stomach are posterior, and the long axis of the fetus is parallel to the long axis of the mother. In this example, the fetal right side would be on the maternal right side. In breech presentation, if the stomach and spine were anterior or “up,” the left side of the fetus would be on the maternal right.
In cephalic presentation with the maternal and fetal axis parallel and the spine and stomach posterior, the fetal left side would be on the mother’s right.


Above. Do a check to make certain that the fetal heart orientation confirms normal situs, situs solitus. The stomach should be on the fetal left side. The fetal spine is closest to the left atrium and the axis of the heart is deviated to the left. The right ventricle is nearest to the anterior chest.
Situs Inversus
Situs inversus occurs when fetal organs which normally occupy one side of the fetus are found on the opposite side. For example, the fetal stomach is found on the fetal right side instead of the normal left side. Similarly, when the right atrium is on the left side and the left atrium is on the right, situs inversus is also defined. When the fetal organs are complete mirror images, situs inversus totalis is defined.


Above. Situs inversus. The fetal stomach bubble is seen on the fetal right side.


Above. Situs inversus. The right atrium is found on the fetal left side and the left atrium is on the fetal right side. This is a fetus with a large ventricular septal defect and other malformations.
Four Chamber View


Above. In this schematic of the fetal four chamber heart [4], the respective chambers are defined as well as the major valve anatomy. Note the direction of the right ventricular outflow tract (RVOT) from right to left and the left ventricular outflow tract (LVOT) initially form left to right. The RVOT crosses over the LVOT.


Above. Apical view. The four chamber view is obtained through a true transverse view of the fetal chest. The right ventricle is closest to the anterior chest wall and the left atrium is closest to the fetal spine. The fetal cardiac apex points to the left chest (levocardia). In a line perpendicular from the mid-line, the fetal cardiac axis is 45 degrees (± 16 degrees).
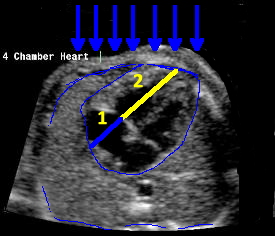

Above. The blue arrows define the path of the ultrasound beam, which is directed transversely to the fetal chest. This is achieved by obtaining a longitudinal view of the thoracic spine and turning the transducer 90 degrees, then moving the transducer towards the fetal head or feet until the above image is obtained. Normally, both atria are similar size and both ventricles are similar size. The ratio between ventricular size and atria size is 2:1. The heart occupies approximate 1/3 of the chest.


Above. Four chamber heart. With normal situs, use the left atrium’s relationship to the spine to determine sidedness of the cardiac chambers. The fetus is in supine position and the border of the right ventricle is under the sternum.


Above. The fetus is supine, the left atrium is nearest to the spine, and the apex of the heart points to the left. The left ventricle occupies most of the left cardiac border.


Above. Four chamber normal fetal heart ultrasound. Again, the left atrium is identified and the atrioventricular valves – the tricuspid valve and the mitral valve – are defined.
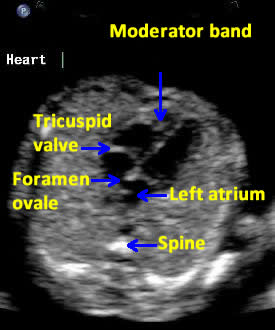

Above. Four chamber heart. The tricuspid valve is inserted towards the apex of the fetal heart compared to the mitral valve. The moderator band is a thick muscle near the apex of the right ventricle. Note the foramen ovale, which opens towards the left atrium.
Interventricular Septum
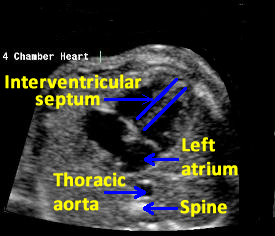

Above. The interventricular septum is the muscular wall that separates and divides the left and right ventricles. It forms part of the crux of the fetal heart and serves as the insertion of the atrioventricular valves.


Above. Long axis view of the interventricular septum is best obtained by a scan plane which is perpendicular to the plane of the septum.
Atrial Views
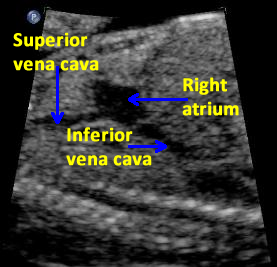

Above. The fetal heart is right side dominant with the well oxygenated blood coming from the umbilical vein through the liver and shunted through the ductus venosus to the inferior vena cava and right atrium. This view of the right atrium with the inferior and superior vena cava is a longitudinal scan plane parallel to the spine and to the right of the fetal heart.


Above. Long axis view of the fetal heart through the atrial septum with the posterior septum secundum and the anterior septum primum. Just to the right of the septum primum is the septum secundum and the valve of the foramen ovale through which well oxygenated blood flows from the right atrium to the left atrium.


Above. Axial view through the four chamber fetal heart demonstrating the right atrium with the leaflets of the tricuspid valve towards the apex and the foramen ovale opening from right to left.


Above. Long axis view of the heart with the transducer perpendicular to the interventricular septum demonstrating the right to left shunt of blood through the foramen ovale.
Pulmonary Veins


Above. Two of the four fetal pulmonary veins are identified. Two inferior and two superior pulmonary veins drain to the left atrium. Sweeping the transducer in a true four chamber view identifies the pulmonary vein.

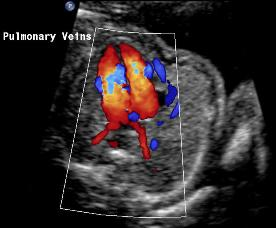
Above. Color Doppler flow demonstrates two pulmonary veins draining to the left atrium.
Left Ventricular Outflow Tract (LVOT)


Above. The left ventricular outflow tract in the fetal heart is seen by obtaining a long-axis view of the heart. The scan head is angled slightly anteriorly and medially (right) from the aortic root. The right ventricle is anterior to the left ventricle. The normal aorta is about 3 mm at 20 weeks. The number of cusps of the aorta should be noted. The aortic motion should be crisp and not “floppy.”


Above. Another view of the left outflow tract showing a typical configuration of the ascending aorta as it exits from the left ventricle.
Right Ventricular Outflow Tract (RVOT)


Above. The main pulmonary artery arises from right to left. The pulmonary valve is demonstrated. From the four chamber view, rock the transducer towards the left fetal shoulder. Again, first obtain a true transverse view of the fetal thorax with the ventricles appearing longer than the atria before changing the direction of the transducer.
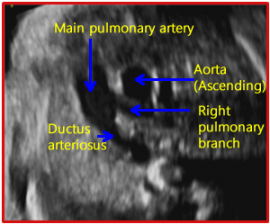
Above. The main pulmonary artery is seen exiting from the right ventricle. Note the ductus arteriosus exiting from the main pulmonary artery and note the right pulmonary branch. The ascending aorta is seen adjacent to the main pulmonary artery.
Above images courtesy of Jill Beithon, RT, RDMS, RDCS, RVT.
Three Vessel View (3VV)
The three vessel view is a transverse view of the fetal upper mediastinum. The views demonstrate in cross section or oblique section the main pulmonary artery, the ascending aorta, and the superior vena cava. [5]
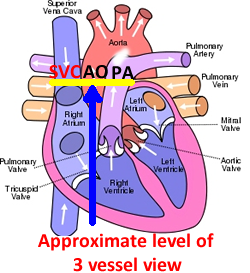

Above. This schematic demonstrates the approximate level of the 3 vessel view, which is a transverse view through the fetal mediastinum. In fetal life, the pulmonary artery is larger than the ascending aorta and superior vena cava, and the typical “dash and 2 dots” demonstrates this relationship.
Above. 3VV. Note the three vessels identified in a transverse view of the fetal mediastinum. The pulmonary artery is anterior and is the largest vessel followed in size by the aorta and the superior vena cava (SVC).

Above. The vessels form a classic visual image of a “dash and 2 dots” with the dash being the pulmonary artery and a part of the ductus arteriosus. Adjacent to the “dash” is the ascending aorta. Adjacent to the ascending aorta is the superior vena cava.
Above. Another 3 vessel view showing the main pulmonary artery, the ductus arteriosus, the ascending aorta, and the superior vena cava. The echogenic structure to the left of the pulmonary outflow is the pulmonary valve.
Above images courtesy of Jill Beithon, RT, RDMS, RDCS, RVT.
Three Vessel Tracheal View (3VT)


Above. The inflow tracts of the superior vena cava (SVC) bring deoxygenated blood to the right atrium and the inferior vena cava brings mostly oxygenated blood from the inferior vena cava (IVC). The oxygenated blood is delivered to the IVC via the umbilical vein to the ductus venosus and the IVC. Again, the views of the inflow tract are best obtained with the transducer longitudinal to the right of the heart and parallel to the fetal spine.
Aortic Arch


Above. The aortic arch arises from the left ventricle. The view is achieved by turning the transducer 90 degrees from a transverse position of the fetal heart to a longitudinal or parasagittal position in the mid-fetal heart. The aortic arch appears as a “candy cane” shape with the head and neck vessels superiorly. Note the ductus venosus and inferior vena cava (IVC).

Above. Another gray scale view of the aortic arch with the parasaggital view also demonstrating the inferior vena cava.
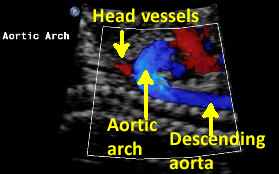

Above. Color Doppler of the aortic arch with a view of the descending aorta and fetal head and neck vessels.

Above. Color power Doppler of the aortic arch with the superior vessels demonstrated.
Commentary and color images above courtesy of Jane JK Burns, RT, AS, RDMS.
Ductal Arch
The ductus arteriosus brings well oxygenated blood from the main pulmonary artery to the descending aorta, and normally closes after birth. The continuity of this vascular connection during fetal life is the ductal arch which is flat, uniform, and slightly larger than the aorta.
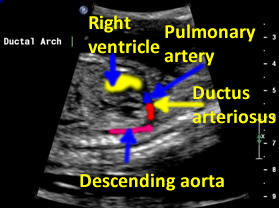

Above. The approximate components of the sagittal view of the ductal arch are: right ventricle, main pulmonary artery, ductus arteriosus, and descending aorta. [6] The shape of the fetal ductal arch is often compared to a “hockey stick.”
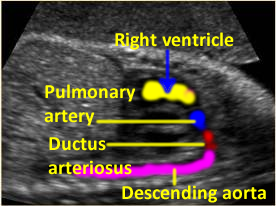

Above. An additional view of the ductal arch demonstrating the major vascular components.

Above. The ascending aorta’s relationship to the aortic arch is demonstrated in this view of the ductal arch.
Color Doppler
Color Doppler adds blood flow information concerning aspects such as perfusion, atresia, and narrowing. Direction as well as detection of flow is possible such as antegrade, retrograde, bidirectional flow and turbulent, shunting, or stenotic flow. Finally, demonstration of small vessels is possible. Color Doppler helps with the placement of the cursor for spectral Doppler applications.
Start with a good 2-D image and use a high frequency transducer. Maintain a parallel orientation to the direction of blood flow. The image quality is affected by the size of the color box, the velocity range, wall filter, persistence, color gain, and color line density. The setting on the 2-D image may need to be reduced. Color persistence may need to be reduced. Initially, low color gain and high PRF (pulse repetition frequency) settings should be used and continuously adjusted as needed. (See below).
Color box size: The size of the color box affects the quality and frame rate. A smaller color box gives a higher frame rate and better image.
Velocity scale or PRF (pulse repetition frequency): affects the quality of the image. A PRF of 45 to 60 cm/sec is optimal for the great arteries and a range of 10 to 20 cm/sec is optimal for venous structures.
Wall filter: eliminates signal from the motion of vessel walls. Select a high filter for the great arteries and a low filter for the pulmonary arteries and the veins.
Persistence: allows overlap of information from the prior images. Use low settings for a cardiac evaluation.
Color gain: reflects the amount of color on the screen. To eliminate artifacts, start with low color gain and adjust as needed.
Color line density: relates to resolution in the axial and lateral planes. If the color line density is increased, the frame rate is decreased. Compromise to obtain the best image quality.
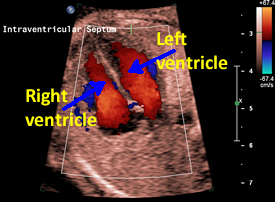
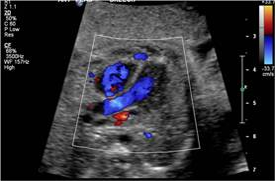
Above. Color Doppler flow demonstrating the ventricles and the interventricular septum and direction of flow with flow towards the transducer (red) and flow away from the transducer (blue).
Above. Color Doppler demonstrating the left ventricular outflow tract. Note the spine in normal situs (situs solitus) orients the direction as to the right side and left side of the fetus. In this instance, the apex of the heart is to the left of the spine and the left atrium would be the nearest to the spine.

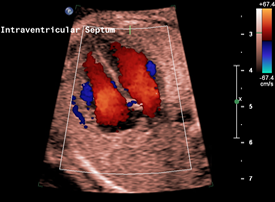
Above. Another color Doppler view demonstrating an intact fetal interventricular septum.


Above. Color Doppler. Flow away from the transducer demonstrates the portion of the aortic arch and thoracic aorta while flow towards the transducer suggests inflow from the inferior vena cava.
Commentary and color images above courtesy of Jane JK Burns, RT, AS, RDMS.