 Search
Search
Transvaginal Ultrasound: Information
Page Links: Introduction, Cervical Length, Preterm Labor, Preterm Labor Prediction, Cervical Length and Twins, Progesterone Supplementation, Threatened Preterm Labor, Other Uses of Transvaginal Ultrasound, References
Acknowledgements and Editorial Advice: Helen Feltovich, MD, MS; Maternal-Fetal Medicine Specialist, Intermountain Healthcare and Associate Research Professor, Medical Physics, University of Wisconsin-Madison.
Image Review: Krista Wald, RDMS, Staff Sonographer, Perinatology Clinics; and Paula Wickham, RDMS, Head Sonographer, Perinatology Clinics: The Mother Baby Center (Allina Health and Children’s Hospitals and Clinics, Minnesota).
Introduction
This chapter is devoted to transvaginal ultrasound (TVUS) of the cervix. It includes a review of cervical length, preterm labor, preterm labor prediction, progesterone supplementation, threatened preterm labor, and other uses of transvaginal ultrasound.
Cervical Length
Transvaginal Cervical Length

Above. The transvaginal ultrasound measurement of cervical length leads to insights into the identification and treatment of a number of important clinical conditions, which range from preterm labor to induction of labor, prolonged pregnancies, timing of repeat C-sections, and management of polyhydramnios. The transvaginal ultrasound technique is superior to transabdominal and/or transperineal cervical length for usefulness and accuracy.
Preterm Labor
Definition
The prevention of preterm labor (PTL) is one of the most important issues facing contemporary obstetrics.

Above. Defined as delivery occurring at less than 37 weeks, the worldwide incidence of preterm birth is 9.6%. [1] Higher rates are reported for Africa and North America and lower rates for Europe. In addition, preterm delivery is responsible for higher rates of neonatal death and morbidity which extend into later life (bronchopulmonary dysplasia, brain injury) [2], and result in increased health care costs.

Above. About 30% to 35% of preterm births are related to medical indications, 40% to 45 % follow spontaneous premature labor, and 20% to 25% follow premature rupture of the membranes. Approximately 40% of preterm births occur at 33 weeks or less gestational age. [3]
Preterm Labor Causation
Spontaneous preterm birth is multifactorial and poorly understood. Regardless of etiology, its varying pathways lead to gross cervical changes commonly associated with early delivery, such as shortening, softening, and dilatation. [4] Solving the problem of preterm birth will require elucidation of molecular and biochemical events underlying the microstructural and biochemical changes that promote preterm birth. [5]
Strategies to Prevent Preterm Labor

Above. A number of strategies are proposed to prevent preterm birth. Preventive measures and interventions are possible. For example, efforts to reduce the frequency of multifetal pregnancies by reproductive health care practitioners and efforts to reduce induction of labor before 39 weeks are associated with reduced preterm births rates. Interventions such as progesterone supplementation and cervical cerclage also reduce the frequency of preterm birth. [6] Other strategies include tobacco control, fertility control, and dedicated prevention clinics. [7]
Preterm Labor Prediction
Cervical Length and Preterm Labor (PTL) Prediction

Above. The detection of a short cervix by transvaginal ultrasound at 18 to 24 weeks gestation is the most powerful predictor of spontaneous preterm birth. [8] In a systematic review among asymptomatic women at increased risk for preterm birth, the most common transvaginal ultrasound cervical cutoff is < 25 mm to predict preterm birth at < 35 weeks gestation. [9] However, other critical cutoff values have been proposed to select women for certain therapeutic interventions.

Above. The cervical length during a normal pregnancy is > 30 mm. A cervical length measured between 14 and 24 weeks gestation of 15 mm or less is associated with a 50% chance of preterm delivery at less than 33 weeks gestation. [10] In women with a prior spontaneous preterm birth, the shorter the cervix, the more likely recurrent preterm birth occurs. When the cervix is < 10 mm, there is a 90% chance of preterm birth before 35 weeks. [11]
Cervical Length and Twins
Is second trimester cervical length (CL) a risk indicator for Cesarean delivery in twins?
In this study, 311 women with a twin gestation attempted vaginal delivery after 34 weeks. Second trimester cervical length was measured in these women to determine if there were an association with the risk of emergency Cesarean section. In nulliparous women, there was no relationship between second trimester cervical length and Cesarean delivery. [12]
Progesterone Supplementation

Above. Hassan and associates reported a 45% reduction in the rate of preterm singleton births before 33 weeks in women who received vaginal progesterone and who had a cervical length of 10 to 20 mm at 19 to 23 6/7 weeks. [13] A meta-analysis of 5 trials suggests that the administration of vaginal progesterone to women with a cervix of ? 25 mm is associated with a reduction in preterm birth at < 28 weeks, < 33 weeks, and < 35 weeks as well as fewer neonatal complications. [14] The natural vaginal progesterone daily dose among the studies was between 90 mg and 100 mg. Presently, formulations and administration routes have not been vigorously tested.
Routine Cervical Length Screening and Progesterone to Prevent Preterm Birth

Above. The ACOG Practice Bulletin on Prediction and Prevention of Preterm Birth in 2012 (confirmed in 2014) recommends that progesterone supplementation should be offered to women at 16 to 24 weeks with a previous singleton preterm birth irrespective of cervical length, and in women who incidentally are noted to have a short cervix of ? 20 mm at or before 24 weeks. [15] While the Bulletin does not mandate universal screening, universal screening “may be considered.” This opinion is consistent with support for universal screening by others. [16] While the option to consider universal screening is open, Iams suggests that programs pursing this path must adhere to cost effectiveness, efficiency, and quality standards to ensure accurate measurements and treatment. [17] The Cervical Length Education and Review (CLEAR) entity is a credentialing program for cervical length measurement offered through the Perinatal Quality Foundation and can be found at: https://clear.perinatalquality.org/.
Finally, for twin and triplet pregnancies, a number of studies show no benefit for progesterone administration in the reduction of preterm labor. [18]
Summary: Critical Cervical Length for Treatment with Progesterone
Given a history of previous spontaneous preterm birth at 16 to 37 weeks, irrespective of cervical length, 17-alpha-hydroxyprogesterone caproate 250 mg is given intramuscularly at 16 to 20 weeks and continued until 36 weeks. [19] If selective or universal screening is undertaken at 18 through 24 weeks and the transvaginal ultrasound cervical length is ? 20 mm, vaginal progesterone is initiated daily with 200 mg capsules or suppositories or 90 mg vaginal gel until 36 weeks. [20]
Threatened Preterm Labor
Tsoi and colleagues found that the transvaginal cervical length (CL) at presentation in singleton women with intact membranes and threatened preterm labor (PTL)predicted delivery within 48 hours, within 7 days, and delivery at < 35 weeks. [21]

Above. When the CL was ? 15 mm no women delivered within 48 hours, and only 0.7% delivered within 7 days. These authors suggest that routine hospitalization may not be necessary in those with threatened preterm labor in the presence of a CL of ? 15 mm. Others also report a CL of ? 15 mm as the most relevant threshold for predicting delivery in women with threatened preterm labor. [22]
While CL is an independent predictor of preterm delivery in women with preterm labor, its predictive accuracy as a single measure is considered relatively limited by some. [23] In addition, the predictive accuracy for CL measurements among women with threatened PTL varies with gestational age at presentation with lower CL cutoff measurements noted at lower gestational ages. [24] Fetal fibronectin (fFn) testing may play a discriminating role in predicting PTL in these women.

Above. In women destined to deliver within 7 days, CL measurements, combined with fetal fibronectin testing improves identification of these women when the CL is between 15 and 30 mm. [25]

Above. The delivery risk between 7 and 14 days in women with threatened premature labor can be assessed by transvaginal CL and fFn performed on day 7 of women hospitalized for preterm birth. [26] The delivery risk between 7 and 14 days was increased in the presence of a CL of < 15 mm or a CL of ? 15 to 30 mm and a positive fFn compared with women with a CL of ? 30 mm.
Preterm Labor and the Risk for Preterm Delivery

Above. After preterm labor is arrested, women are at increased risk for preterm delivery if the cervix is ? 1 cm dilated by digital exam, < 15 mm CL on transvaginal ultrasound, and/or a positive fFn. [27]
Preterm Delivery Calculator

Above. The Center for Medical Statistics, Informatics, and Intelligent Systems (CeMSIIS) has created a statistical prediction model for individualized assessment for the risk of preterm delivery within 48 hours after transfer and before 32 weeks of gestation. [28] Data for the online calculator include: fetal fibronectin, transvaginal cervical length in mm, and C-reactive protein. A disclaimer is provided. This calculator can be accessed at the following link: CeMSIIS
See also QUiPP for preterm birth calculator information.
Low Risk for Preterm Delivery
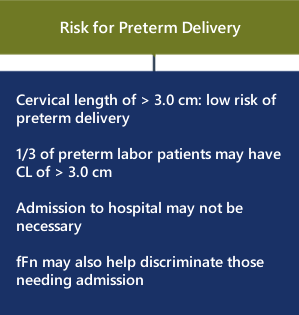
Above. Women with a transvaginal cervical length of 3.0 cm or greater are unlikely to deliver prematurely despite admission for threatened premature labor. Over 1/3 of women with CL of > 3.0 cm are admitted unnecessarily to some hospital units with preterm labor. Yet, few or none deliver prematurely leading to inconvenience and cost. [29] The addition of fetal fibronectin testing in these women may be cost effective. [30]
Other Uses of Transvaginal Ultrasound
Cervical Cerclage and Preterm Delivery
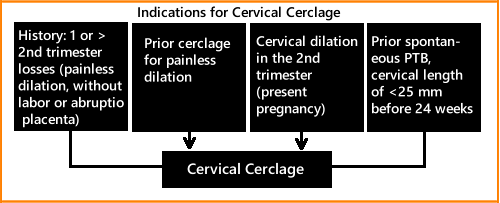
Above. The ACOG Practice Bulletin on Cerclage for the Management of Cervical Insufficiency in 2014 suggests cerclage placement may be indicated in women with a singleton pregnancy who have a history of one or more second trimester pregnancy losses with painless dilatation and without labor or abruption placenta, history of prior cerclage for painless dilatation, and physical examination of cervical dilatation in the second trimester. [31] In addition, patients with prior spontaneous preterm birth, transvaginal cervical length of < 25 mm before 24 weeks may be candidates.
In a review of 5 randomized controlled trials, there is no evidence that cerclage is effective in multiple gestations in preventing preterm births, or in reducing perinatal deaths or neonatal morbidity. [32]
Cervical Length and Induction of Labor

Above. The cervical length and Bishop score are significant predictors of successful induction of labor. Patients who deliver within 24 hours demonstrate a mean cervical length of 23.1 mm compared to women who deliver after 24 hours, who demonstrate a mean cervical length of 31.3 mm. [33] An independent predictor of C-section is a cervical length of 20 mm at the time of induction of labor at term. [34]
Transvaginal ultrasound of 1571 singleton low-risk pregnancies at 37 weeks predicted the onset and outcome of labor. [35] Women with a cervical length of 10 mm delivered at a mean gestation of 38 weeks, while those with a cervical length of 35 mm delivered at 41 weeks.
The following charts from the study’s abstract summarize the findings:

Above. Longer transvaginal cervical lengths measured at 37 weeks are associated with a higher incidence of delivery after 40 weeks and 10 days.

Above. Longer transvaginal cervical lengths measured at 37 weeks are associated with a higher rate of C-sections for failure to progress.
Cervical Length and Prolonged Pregnancy

Above. The chance for spontaneous labor at 41 weeks is greater in white, parous women and is greater when the maternal body mass index (BMI) is lower and when the sonographic cervix length is shorter. Further, these factors can define the probability of spontaneous labor and the risk of C-section in the week following the 41st week of pregnancy. [36]
In women undergoing induction of labor at 41 3/7 weeks to 42 1/7 weeks, a shorter sonographic cervical length and multiparity predicted the induction to delivery interval and the likelihood of vaginal delivery within 24 hours. [37]

Above. Transvaginal cervical length in women undergoing induction of labor at 41 3/7 to 42 1/7 weeks and the percent of those delivering within 24 hours according to parity. [38]
Cervical Length and Polyhydramnios

Above. There is a gradual shortening of cervical length in women with polyhydramnios and a cutoff of 15 mm was associated with a lower gestational age at delivery. [39]
References
-
Abstract: PMID: 20428351 -
Abstract: PMID: 17762416 -
Abstract: PMID: 18177778 -
Abstract: PMID: 22717270 -
Abstract: PMID: 25084285 -
Abstract: PMID: 24806178 -
Abstract: PMID: 25477878 -
Abstract: PMID: 21879816 -
Abstract: PMID: 18412093 -
Abstract: PMID: 10871466 -
Abstract: PMID: 20708169 -
Abstract: PMID: 25402630 -
Abstract: PMID: 21472815 -
Abstract: PMID: 22284156 -
Abstract: PMID: 22996126 -
Abstract: PMID: 21472815 -
Abstract: PMID: 24807317 -
Abstract: PMID: 25731690 -
Abstract: PMID: 22996126 -
Abstract: PMID: 24807317 -
Abstract: PMID: 15736212 -
Abstract: PMID: 24342367 -
Abstract: PMID: 24201691 -
Abstract: PMID: 24907701 -
Abstract: PMID: 24807328 -
Abstract: PMID: 25845495 -
Abstract: PMID: 24839150 -
Abstract: PMID: 25616254 -
Abstract: PMID: 23816842 -
Abstract: PMID: 23791688 -
Abstract: PMID: 24451674 -
Abstract: PMID: 25208049 -
Abstract: PMID: 25123514 -
Abstract: PMID: 17444553 -
Abstract: PMID: 14689532 -
Abstract: PMID: 18816476 -
Abstract: PMID: 12858301 -
Abstract: PMID: 12858301 -
Abstract: PMID: 17019742