 Search
Search

Please note: the course must be completed before you attempt the quiz.
After completing the course, to take the quiz: Click Here
This course contains the following topics:
Placenta Accreta
Placenta Previa
Placenta Accreta: Information
Page Links: Definition, Underlying Pathology, Clinical Problem, Incidence and Risk Factors, C-Section/Previa Relationships, MRI and Other Diagnostic Methods, Sonographic Features, Maternal Outcomes, Triple-P Procedures, Balloon Catheters for Placenta Accreta, Conservative Management, References
Definition
Placenta accreta is a general term for abnormal placental attachments. The term denotes a spectrum of attachment disorders, usually defined as: placenta accreta, placenta increta, and placenta percreta.

Above. Normal ultrasound. 2-D gray scale shows an area of decreased echoes between the placenta and the uterine wall near the area of the decidua basilis.


Above. Placenta accreta or placenta accreta vera. The placenta invades the decidua basalis and attaches abnormally to the myometrium.


Above. Placenta increta. The placenta invades into the myometrium (uterine wall).


Above. Placenta percreta. The placenta penetrates through the wall of the uterus to the surface or serosa of the uterus. The placenta may also penetrate the sidewalls of the uterus (parametrial), or into the maternal bladder.
Underlying Pathology

Above. The pathology of placenta accreta is related to a defect in the decidua basalis caused by uterine scaring [1], and a variety of surgical procedures may be responsible for the defect.

Above. The recent increase in cesarean birth and repeat cesarean births increase the overall incidence of anterior uterine scarring. [2] These trends translate into a significant effect on the incidence of placenta accreta.
Clinical Problem
In summary, a low-lying placenta or placenta previa may implant over a previous C-section scar and result in myometrial invasion, which can be associated with major maternal hemorrhage at the time of birth. [3] The hemorrhage is a result of incomplete separation of the placenta from the uterine wall.


Above Left. Placenta increta. Cut hysterectomy specimen demonstrating penetration of placental tissue into the uterine wall. Note placenta that remained in situ.
Above Right. Placenta increta. This view demonstrates the cut uterine surface and shows the penetration of the placenta into the uterine wall. Both placental tissue and placental membranes are adherent to portions of the uterine muscle.


Above Left. Placenta increta. Microscopic examination of the uterine specimen shows invasion of the chorionic villi (placental tissue) into the myometrium.
Above Right. Microscopic examination of the uterine specimen. Note the relationship of the chorionic villi (placental) tissue to the uterine muscle (myometrium).
Incidence and Risk Factors

Above. The incidence of placenta accreta is recorded according to recent studies and varies from almost 0.5% to almost 1%. [3],[4],[5].
The incidence has progressively increased as the number of C-sections have increased. Placenta accreta is one of the greatest challenges in contemporary obstetrics.

Above. Most patients with placenta accreta will demonstrate one or more risk factors [3] and, as expected, the highest risk factors are placenta previa and C-sections.
Other risk factors are defined and include: multiparity [4], previous curettage [4], history of myomectomy [6], endometrial ablation [7], hysteroscopy lysis of adhesions [8], and termination of pregnancy (unknown effect). [9]
C-Section/Previa Relationships
As noted previously, the combination of previous cesarean sections and anterior placenta previa demonstrates a high association with placenta accreta. [10],[11]
In patients with placenta previa, the correlation is strong between the number of previous cesarean deliveries, and placenta accreta and peri-partum hysterectomy. [12]

Above. An observational study of 30,132 patients demonstrates the associations between the number of previous cesarean sections (in the presence of placenta previa) and placenta accreta. [13]

Above. In patients without the presence of placenta previa, the association is demonstrated between the number of previous cesarean deliveries, placenta accreta, and peri-partum hysterectomy. [12]
Approximately 78% of the time, placenta accreta is associated with one prior cesarean birth, and approximately 88% of the time, placenta accreta is associated with placenta previa. [14]
In addition, the risk for placenta accreta is increased in patients with complete placenta previa, after controlling for other factors. [15]

The likelihood of placenta increta or percreta is dependent upon whether or not there is a history of previous C-section. [16] If there is a combination of prior C-section and placenta previa, 37% of patients are likely to exhibit either placenta increta or percreta. [16]
In patients with placenta previa alone, and no prior history of C-section, the likelihood of placenta increta or percreta is low (1.1%).


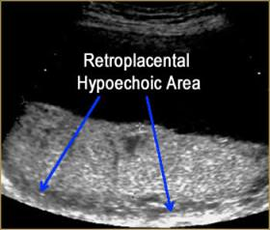
Above. The presence or absence of the retroplacental clear space is not a reliable finding for the ultrasound diagnosis of placenta accreta. Using this criterion is responsible for a high number of false positives (54.5%). [17] In the images above, this is demonstrated. Although a retroplacental space is present, this patient is at risk for placenta accreta due to the findings of anechoic spaces and lacunae.
MRI and Other Diagnostic Methods

Above. Two-stage ultrasound followed by MRI was studied in 453 patients with risk factors for placenta previa, previous cesarean section, and low-lying anterior placenta. In this study, sensitivity and specificity was found to be similar between ultrasound and MRI. [18]

Above. The main MRI findings for placenta accreta are outlined. [19] Thinning of the uterine wall is another principal finding [20], while dynamic contrast MRI may differentiate chorionic villi from decidua basalis. [21]

Above. Findings and potential benefits are outlined for patients undergoing MRI (N = 252). [22] The greatest value of an MRI is in identifying the presence of parametrial invasion and the depth of placental invasion. In suspected percreta, an MRI is warranted. Bladder wall assessment can be made directly by cystostopy.
Computed Tomography: CT has a limited role in the evaluation of placental accreta due to radiation risks. [23]

Above. Vascular endothelial growth factor (VEGF) and placental growth factor (PGF) have been studied in placentas with accreta and controls. [24] Up-regulated VEGF and down-regulated VEGFR-1 may be associated with the development of placenta accreta. In addition, up-regulated angiopoietin-2 and down-regulated Tie-2 may play a role in the development of placenta accreta. [25]

Above. Other potential biomarkers for placenta accreta include: 1). Cell-free DNA. 2). Placental base MRNA. 3). DNA micro. [26] These biomarkers may be identified in maternal blood and could serve as a prenatal screening method for placenta accreta. However, at this time, clinical history, symptoms, and current imaging modalities are the mainstays for diagnosis.
Diagnostic and Sonographic Features
Recent papers have reviewed and clarified diagnostic and sonographic features of placenta accreta.
The overall sensitivity of sonography for placenta accreta diagnosis is 86.4% versus 84% for MRI.
The following is noted during the first trimester [27]:
1. The presence of a lower uterine segment gestational sac.
2. Presence of irregular vascular spaces within the placenta.
3. Implantation of gestational sac within a lower uterine scar.
During the second and and third trimester, the following are possible findings [28]:
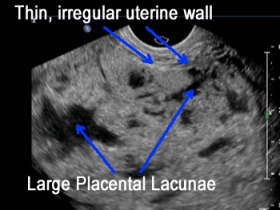
1. Multiple vascular lacunae within the placenta.
2. Loss of retroplacental hypoechoic zone.
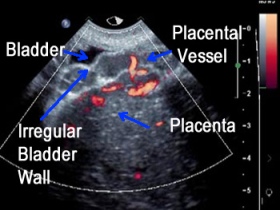
3. Abnormalities of the interface between the bladder and uterine serosa.
4. Villi extension into myometrium, serosa, or bladder.
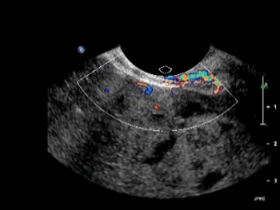
5. Doppler demonstration of turbulent flow through lacunae.
When multiple observers are blinded from sonographic patients with and without placenta accreta, the diagnostic accuracy ranges from 55.9% to 76.4% with sensitivities from 53.4% to 74.4%, and overall, inter-observer agreement is moderate. [29]
Maternal Outcomes
Placenta accreta is a common indication for peripartum hysterectomy. [30] Maternal adverse outcomes include hemorrhage and its attendant morbidity.

Above. The graph reviews 4 studies and demonstrates the percentage of patients undergoing peripartum hysterectomy as a result of placenta accreta.
The overall incidence of peripartum hysterectomy is .8 to .4 per 1000 deliveries, but the most common indication is placenta previa/accreta. [31],[32] In some series, 50% of peripartum hysterectomies are due to placenta accreta or a variant, while others report 20% for accreta and 56% for uterine atony. [33] The overall incidence of peripartum hysterectomy has declined, while placenta accreta as an indication has increased significantly. [34]
Maternal outcomes from peripartum hysterectomy include: maternal death 4%, urinary injury 15%, relaparotomy 25%, > 10 units of packed cell transfusion 67%, and ICU admission 77%. [11]
Others report: cardiac arrest, intravascular coagulopathy, pulmonary edema, septicemia, and bladder injury. [28]
Maternal mortality is reported as high as 16.7% when mothers are transported from rural areas with major hemorrhage due to placenta accreta. Planned rather than emergent hysterectomy results in less morbidity. [35]
The Triple-P Procedure
A recent article “Prevention of postpartum hemorrhage and hysterectomy in patients with morbidly adherent placenta: a cohort study comparing outcomes before and after introduction of the Triple-P procedure” discusses the efficacy of the Triple-P procedure. [36] The Triple-P procedure is a surgical method intended to reduce postpartum hemorrhage and hysterectomy in cases of placenta accreta, including placenta increta and percreta. Step 1 involves placental localization and delivery of the fetus via a transverse uterine incision above the upper margin of the placenta. Step 2 involves the inflation of preoperatively placed occlusion balloons into both internal iliac arteries. In Step 3, the placenta is not separated and myometrial excision and reconstruction of the uterine wall is performed. If the bladder is invaded (percreta), the placenta is left in situ and hemorrhagic areas are treated with hemostatic powder. The Triple-P procedure resulted in reduced hysterectomy, postpartum hemorrhage, and hospital stay among a small cohort of patients. The authors acknowledge the need for further multicenter studies to confirm improved outcomes. Further, this procedure should be attempted only in centers with high levels of expertise among multiple disciplines. [37]
Balloon Catheters for Placenta Accreta
A recent article “Precesarean prophylactic balloon catheters for suspected placenta accreta: a randomized controlled trial” [38] addresses a study of twenty seven women that were randomized to an intervention group (13) who underwent prophylactic balloon catheter placement for suspected placenta accreta and 14 control patients who did not undergo placement. The outcome measure was the number of packed red blood cell units transfused, which did not differ between the two groups. Two of 13 women (15.4%) in the treatment group had reversible adverse effects. This is one of the few studies to address this issue. The authors acknowledge the small sample size and emphasize the difference between prophylaxis and treatment of postpartum hemorrhage by arterial embolization, which has been shown to be effective.
Conservative Management
Conservative management of placenta accreta is defined as leaving the placenta in situ under one or more of the following approaches:
• 1. without additional interventions.
• 2. adjuvant methotrexate.
• 3. selective arterial embolization.
Since morbidity is potentially high, conservative management is usually considered when:
• 1. blood loss is minimal, and
• 2. fertility preservation is desired. [39]
In a 20-year literature review, 60 women underwent conservative management. In this study, 26 women were managed without any other intervention. In 19 of 26 patients, the placenta had been partially removed. In 4 of these 26, conservative therapy failed. In 19 of 22 women in whom the placenta was left in situ and who received adjuvant methotrexate, 5 of 22 failed conservative therapy. Three of 12 failed therapy when arterial embolization was used as an adjuvant. [32] Overall, 11 of 60 patients suffered infection, 21 of 60 had hemorrhage, and 4 of 60 had disseminated intravascular coagulation (DIC). [32]

Above. This chart represents the overall morbidity of 60 patients with placenta accreta who were treated conservatively. [32]
A historical comparison of conservative versus radical treatment of placenta accreta demonstrated a reduction in blood loss, hysterectomies, and DIC in patients treated conservatively. [40] Finally, fertility was preserved in 3 of 50 who were conservatively managed for placenta accreta, although either medical or surgical therapy was necessary in 70%. [41]
Conservative treatment of placenta accreta can result in prolonged retention of the placenta and delayed postpartum hemorrhage. Alternatively, hysteroscopic resection has been reported as one method of management. [42]
For radical treatment of placenta accreta, some studies demonstrate no benefit from prophylactic placement of intravascular balloon catheter [43],[44], while the possibility of morbidity, including iliac artery thrombosis and limb ischemia, has been reported. [45]
In cases that do not require hysterectomy, placement of intrauterine balloon compression and intrauterine packing may be successful in experienced hands as a means to control hemorrhage.
In women with a history of multiple C-sections and who do not desire further fertility, consultation and informed consent is warranted regarding planned cesarean hysterectomy. Proper anesthesiology and blood banking consultation can be obtained and allied personnel engaged. Placement of ureteral catheters and cystoscopy to assess for bladder invasion can be performed in the immediate preoperative period. Prior to the procedure, ultrasound can define the limits of the placenta and a fundal hysterotomy incision can be made for safe delivery of the baby. Strict hemostasis is maintained by over-sewing the hysterotomy site. The placenta can be left in situ while deliberate and careful hysterectomy is performed under controlled circumstances.
Placenta Accreta: Imaging Considerations
Early Diagnosis of Placenta Accreta
At 10 weeks or less, ultrasound demonstrates:
• Gestational sac in lower uterine segment.
• Implantation of the sac over the uterine scar. [46]
At 16 weeks or greater, ultrasound demonstrates:
• Irregularly shaped vascular sinuses with color Doppler.
• Irregular or small bulge into the adjacent bladder.
• Placental sinuses that cross the bladder wall. [47]
Transvaginal ultrasound and color Doppler imaging improve the accuracy of placenta accreta prediction in patients at risk. [48]
The highest positive predictive value for placenta accreta is irregular vascular spaces within the placenta (placenta lacunae). [49]
Summary
In patients with previous C-section, ultrasound findings for placenta accreta include:
1. Gray scale 2-D: multiple venous lakes (lacunae).
2. The presence or absence of lacunae is important in assessing the risk for maternal hemorrhage. No hysterectomies are performed when lacunae are absent. [50][51]
3. Color Doppler: vascularity with abnormal vessels linking placenta to bladder [52] and placenta to myometrium.
4. Finally, less than 1 millimeter for myometrium thickness is associated with placenta accreta. [53]
Placenta Accreta: Images


Above. Transvaginal ultrasound image in patient with previous C-section and placenta. Note small lacunae and and the placental location over the internal cervical os (complete placenta previa).

Above. Transvaginal ultrasound demonstrates placental lacunae in a patient with placenta accreta.

Above. Note precise color Doppler imaging demonstrates increased vascularity. There is increased vascularity and penetration of placental vessels to the myometrium.


Above. Color Doppler imaging demonstrates increased vascularity, and potential penetration of placental vessels to the myometrium.


Above. Note relatively smaller lacunae in a patient at risk for placenta accreta.


Above. Note relatively thin myometrium of 1.8 mm in a patient at risk for placenta accreta.

Above. Note the thin uterine wall and the large lacunae suggestive of placenta accreta.
Placenta Accreta: Video
Above. Patient 1. Anterior placenta previa with lacunae suggesting placenta accreta. The placenta is implanted in the lower uterine segment and covers a previous C-section scar.
Above. Patient 1 (continued). Note the well-defined lacunae and the relationship of the low-lying anterior placenta to the lower uterine segment.
Above. Patient 1 (continued). Placenta accreta. Color Doppler demonstrating vascular flow between the placenta and the lower uterine segment. The color settings are not sufficient to demonstrate vascular penetration between the placenta and the uterine wall.
Above. Patient 2. Placenta accreta. 2-D gray scale demonstrating anterior placenta previa overlying a previous C-section scar. Note multiple placental lacunae.
Above. Patient 3. Placenta accreta. Color flow Doppler. Note anterior placenta with large lacunae. The uterine wall is thin and color flow suggests penetrating vessels from the placenta to the uterine wall.
Above. Patient 4. Placenta accreta. Color flow Doppler. The placenta and uterine wall are well-defined. The color flow settings are effective in demonstrating penetrating vessels from the placenta to the uterine wall.
Above. Patient 5. Placenta accreta. Color power Doppler. Again, the placenta and uterine wall are well-defined and the color power settings suggest penetration of placental vessels to the uterine wall.
Above. Patient 6. Placenta accreta. Color power Doppler. The placenta is separate from the thickened anterior uterine wall and the maternal bladder is noted separately. Vascular penetration is demonstrated between the placenta and the uterine wall.
Placenta Previa: Information
Page Links: Definition, Incidence, Risk Factors, Placental “Migration”, Symptoms, Outcome, Clinical Summary, References
Definition
Placenta previa is a placental implantation abnormality when any portion of the placenta covers or is near the internal cervical os.
Previous definitions include 3 groups:
• Complete placenta previa: the placenta covers the entire cervical os.
• Partial placenta previa: the edge of the placenta partially covers the internal cervical os.
• Marginal placenta previa: the placenta is at the margin of the internal cervical os but does not cover it.
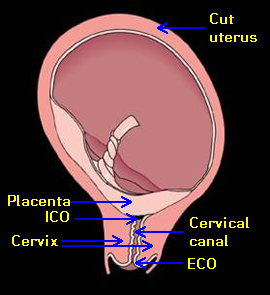

Above. This cut diagram of the uterus with complete placenta previa demonstrates the critical relationships between internal cervical os (ICO), the cervix, and the placenta. The cervical canal is illustrated as well as the external cervical os (ECO).


Above. Note the placenta partially covers the internal cervical os and is within 2 cm of the internal cervical os (ICO), but does not completely cover the os.
Transvaginal ultrasound permits accurate measurement of the distance between the internal cervical os and placental edge. Definitions include the following:
Complete placenta previa: the placenta covers the internal cervical os.
Incomplete placenta previa: the leading edge of the placenta is within 2 cm of the internal os.
Low-lying placenta: the placenta is greater than 2 cm from the internal cervical os, but is in the lower 1/3 of the uterus.
Incidence

While the incidence varies by parity [54], the overall incidence is about 4.4 per 1000 births. [55]

Some reports suggest that the incidence is dependent upon a history of prior C-section [56], but prediction models for women with a history of 1 prior C-section show a low sensitivity (13%). [57] In addition, the odds ratio of 1.4 (95% CI 1.1,1.6) shows only a moderate risk for placental abruption and placenta previa as a long-term effect of previous C-section [58], while others show no predictive value of previous C-section for detecting placenta previa based upon a second trimester ultrasound scan. [59]
Risk Factors

Risk factors for placenta previa are subdivided into historical and present pregnancy categories. [60]
• Risk of placenta previa is nearly 3 times higher in pregnancies following assisted reproduction. [61]
• Rate of placenta previa is 40% higher among twins than singletons. [62]
Placental “Migration”

The apparent leading edge of the placenta may “migrate” from the lower uterine segment away from the region of the internal cervical os.
• Longitudinal ultrasound studies [63] demonstrate that the incidence of low-lying placenta is about 15% at 12 to 14 weeks gestation. However, 85% of these early abnormal placental implantation sites revert to normal by term.
• At 30 weeks gestation: 60% of partial placenta previas persist to term.
• At 30 weeks gestation: 75% of total placenta previas persist to term.
However, there is a greater persistence to term if there is a complete placenta previa or posterior placenta previa within 1 cm of the internal cervical os (ICO) [64], and a final placental distance of < 2.0 cm is associated with C-section and peripartum complications. [65]
Symptoms
The classic symptom of placenta previa is painless vaginal bleeding.
• Overall, the incidence of genital bleeding at > 24 weeks gestation is 2% to 5%. [66]
• Outcome is generally better for women with a history of light vaginal bleeding occurring between 16 and 24 weeks compared to women with heavy bleeding. Prognosis is worse in placenta previa patients with heavy bleeding. [67]
• Placenta previa patients have higher rates of [68]:
Second trimester bleeding (OR* 156.0, 95% CI** 87.2-277.5)
Abruptio placenta (OR 13.1, 95% CI 8.2-20.7)
Placenta accreta (OR 3.6, 95% CI 1.1-9.9)
Postpartum hemorrhage (OR 3.8, 95% CI 1.2-10.5)
Postpartum anemia (OR 5.5, 95% CI 4.4-6.9)
*OR=odds ratio; ** CI=confidence interval
Outcome

Increased use of transvaginal ultrasound increases diagnostic precision and links findings to potential clinical outcomes.
Sonographic features predictive of massive bleeding include [69]:
• Echo-free space in the lower edge of the placenta overlying cervix.
• Placental “lacunae.”
• Sponge-like echoes in adjacent uterine wall.
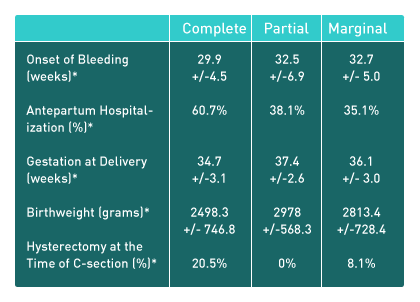
All outcomes: partial placenta previa did not differ from marginal placenta previa.
Women with complete placenta previa had significantly poorer outcomes compared to the other 2 groups.
Others show that pregnancy outcomes vary with the type and designation of placenta previa. [70]
The risks for complete placenta previa are greater than those of incomplete placenta previa and include an increased risk for the following [71]:
• Antepartum and postpartum transfusions
• Postpartum hemorrhage
• Postpartum hysterectomy
• Placenta accreta
• Low birth weight
Low-lying placenta:
Postpartum hemorrhage is the main adverse outcome for patients with low-lying placenta detected during the second trimester of pregnancy.
Clinical Summary
Placenta Previa Summary (based upon the above literature review).
Placenta previa definitions:
Complete placenta previa: the placenta covers all of the internal cervical os.
Incomplete placenta previa: the placenta is within 2 cm of the internal cervical os.
These changes in definition are due to the following factors:
• The accuracy of transvaginal ultrasound in defining the relationship between the leading placental edge and the internal cervical os.
• Poorer outcomes are reported for complete placenta previa compared to partial and marginal placenta previa.
• The apparent non-difference in outcomes between partial and marginal placenta previa.
The incidence of placenta previa is from 1.9 to 3.9 per 1000 live births and is dependent upon parity and possibly upon a history of prior C-section.
Risk factors for placenta previa are:
• Historical: Prior C-section, pregnancy termination, increased parity, maternal age.
• Present pregnancy: Assisted reproduction, smoking, multi-fetal gestation.
• Symptoms/Associations: The primary symptom is genital bleeding, which occurs in 2% to 5 % of pregnancies at > 24 weeks and outcome is based upon the severity of bleeding.
Patients with placenta previa have higher rates of:
• Second-trimester bleeding
• Abruptio placenta
• Placenta accreta
• Postpartum hemorrhage
• Postpartum anemia
Placental “migration”:
• The findings on early ultrasound persist to term in only a small number of patients with a low-lying placenta or placenta previa.
• At 28 weeks and beyond, continued placental migration persists into the third trimester in some patients.
• At 28 to 32 weeks, complete placenta previa or posterior placenta previa within 1 cm of the internal cervical os (ICO) tends to persist.
Outcomes:
Ultrasound findings predictive of massive bleeding include:
• Echo-free space in the lower edge of the placenta overlying the cervix.
• Placental “lacunae.”
These findings are also associated with placenta accreta and explain their overlying relationship and significance for bleeding.
Placenta Previa: Imaging Considerations
Carefully assess patients with risk factors, especially those with:
1. Prior history of C-section, pregnancy termination.
2. Increased parity, advanced maternal age, and assisted reproduction.
Transabdominal Ultrasound
The lower uterine segment, the placenta, and internal cervical os (ICO) should be imaged by 20 weeks with the transabdominal ultrasound probe. On the transabdominal scan, the lower uterine segment images can be obtained by a sagittal view showing the internal cervical os in relationship to placental tissue. Transvaginal ultrasound should be performed if the relationship between the placental edge and the ICO is not clear. In some cases, fluid or clot may be adjacent to the ICO, supporting the need for transvaginal ultrasound.


Above. Transabdominal ultrasound. Sagittal view. Anterior placenta extending to the lower uterine segment and to the region of the internal cervical os. A mixed pattern of echogenicity suggests the presence of fluid/clots, which is consistent with the clinical history of bleeding.
Transvaginal Ultrasound
The probe should be activated at the beginning of the transvaginal exam. Complete information can be obtained without the probe touching the cervix. The transvaginal image should demonstrate the internal cervical os (ICO), the external cervical os (ECO), and the endocervical canal. In addition, a measurement of the cervical length should be obtained. In the midline sagittal plane, the placenta and the placental margin should be identified and measurements taken between the leading edge of the placenta and the internal cervical os.


Above. Transvaginal ultrasound. Sagittal view. Note the internal cervical os (ICO), the external cervical os (ECO), and the cervical canal. Measurements in centimeters should be obtained of the cervical length and the distance between the placental margin and the internal cervical os.
Using the measurements between the margin of the placenta and the internal cervical os obtained by transvaginal ultrasound, only three relationships need to be reported between the placenta and internal cervical os:
1. Complete placenta previa: the placenta completely covers the internal cervical os.
2. Incomplete placenta previa: the leading edge of the placenta is within 2 cm of the internal os.
3. Low-lying placenta: the placenta is greater than 2 cm from the internal cervical os, but is in the lower 1/3 of the uterus.
In addition, if echoes are consistent with blood, free fluid, or clot, these findings should be described and reported. Assessment for placenta accreta is important in patients with a prior C-section or uterine scar; such findings include multiple lacunae, a hypoechoic line between placenta and bladder, and sub-placental zones. The presence of a velamentous cord insertion and accessory placental lobes increase the risk for a fetal vessel crossing the internal cervical os (vasa previa).
Transabdominal Ultrasound
Errors in identifying placenta previa include: inability to distinguish the anatomic lower uterine segment and inability to define the region of the internal cervical os. The fetal position may obscure a posterior low-lying placenta or posterior placenta previa, as the fetal head may be displaced superiorly. Uterine contractions and maternal bladder filling may contribute to a false positive diagnosis.
Effect of maternal bladder filling:


Above. This schematic demonstrates the effect of overfilling the maternal bladder in relationship to a potential posterior placenta previa. When the maternal bladder is overfilled, the lower uterine segment is displaced, and there is no evidence of placenta previa. When the maternal bladder is decompressed, the possibility for a posterior placenta previa exists, and transvaginal ultrasound is indicated.
Effect of uterine contraction:


Above. Uterine contractions can distort the anatomy of the lower uterine segment and cervical area.
A prolonged lower-segment uterine contraction demonstrates no evidence of placental tissue near the internal cervical os. The fetal head is demonstrated in its normal anatomic position.


Above. Same patient during the same scan session. The contraction has dissipated, and placental tissue is observed in close approximation to the internal cervical os.
Placenta Previa: Images


Above. Patient 1. Transabdominal ultrasound, 20 weeks. Sagittal view. Note placental tissue near the ICO (internal cervical os) and note the ECO (external cervical os) at the proximal end of vagina. A lower uterine segment contraction appears present.


Above. Patient 1 (continued). Transabdominal ultrasound, 20 weeks. Sagittal view. The uterine contraction is no longer present and a better distinction is appreciated between the placental margin and the ICO (internal cervical os). Note the umbilical cord is in the lower uterine segment but there is no evidence for umbilical vessel crossing near the internal os. Transvaginal ultrasound is indicated, but at this gestational age, regression of the placental margin by term is likely.


Above. Patient 2. Transabdominal ultrasound, 20 3/7 weeks. Sagittal view. The placental margin is near the ICO (internal cervical os). The mixed echogenic pattern in the lower uterine segment is fluid/clot, again consistent with maternal bleeding.


Above. Patient 3. Transabdominal ultrasound, 20 5/7 weeks. Sagittal view. Note placental tissue and margin are near the ICO (internal cervical os). The exact arrangement between placental margin and ICO is not known and a transvaginal ultrasound is indicated.


Above. Patient 3 (continued). Transvaginal ultrasound, 20 5/7 weeks. Sagittal view. The transvaginal ultrasound clearly defines the ICO (internal cervical os) and the margin of the placenta allowing precise measurement between the placental edge and the ICO. The 2.1 cm measurement at this gestational age is reassuring, but follow-up transvaginal ultrasound at approximately 28 to 30 weeks is warranted.


Above. Patient 4. Transvaginal ultrasound. Sagittal view. The distance between the ICO and placental margin is 1.35 cm. This would qualify as a designation for incomplete placenta previa or marginal placenta previa and both clinical and ultrasound follow-up is warranted.


Above. Patient 5. Transvaginal ultrasound. Sagittal view. The margin of the placenta completely covers the ICO (internal cervical os). At advanced gestational ages (28 to 30 weeks), this finding may not regress. At earlier gestational ages, there is the possibility of regression. However, in either case, both clinical and transvaginal ultrasound follow-up are warranted.


Above. Patient 6. Transvaginal ultrasound. Sagittal view. The margin of the placenta completely covers the ICO (internal cervical os). Total placental thickness extends from the ICO to the margin of the cervix. This finding is unlikely to regress irrespective of gestational age and again, warrants close clinical and ultrasound follow-up. The designation would be complete placenta previa.


Above. Patient 6 (continued). Transvaginal ultrasound. Sagittal view. Complete placenta previa with the placenta completely covering the ICO and the cervix.


Above. Patient 6 (continued). Transvaginal ultrasound. Sagittal view. Complete placenta previa with the placenta completely covering the ICO and the cervix. The placenta extends to the lower uterine segment both anteriorly and posteriorly.


Above. Patient 7. Transvaginal ultrasound. Sagittal view. Note a portion of the placenta covers the ICO. In addition, there is an anechoic area near the ICO. Without color Doppler flow, it is not possible to distinguish whether the anechoic area represents blood fluid or clot or whether it is a vascular structure.


Above. Patient 7 (continued). Transvaginal ultrasound. Sagittal view. Color Doppler flow clarifies the nature of the anechoic area seen on 2-D ultrasound. These structures are vascular and represent placental vessels. These vessels are likely the origin of the massive maternal bleeding, which can sometimes occur with placenta previa.
Placenta Previa: Video
Above . Transabdominal sagittal scan of possible placenta previa. The placental margin extends to the lower uterine segment near the region of the ICO (internal cervical os). Transvaginal ultrasound is necessary to accurately assess the relationship between placental margin and ICO.
Above. Transabdominal ultrasound demonstrating the lower uterine segment and the region of the ICO (internal cervical os). The UC (umbilical cord) is noted in the lower uterine segment, but the umbilical cord vessels do not separately cross the ICO. The findings do not suggest vasa previa.
Above. Transvaginal ultrasound demonstrating complete placenta previa. The ICO (internal cervical os) and cervix are completely covered by placental tissue. Under these circumstances, there is little likelihood of placental regression.
Above. Transvaginal ultrasound demonstrating complete placenta previa. In addition, there are spaces or lacunae within the placenta which suggest the possibility of placental invasion into the myometrium (placenta accreta).
Above. Color Doppler flow in placenta previa. The placenta completely covers the ICO (internal cervical os) and color Doppler demonstrates PV (placental vasculature). These vessels are of maternal origin and constitute a part of the placenta. Rupture of such vessels with placental separation can be responsible for maternal hemorrhage.
References
After completing the course, to take the quiz: Click Here.
-
Abstract: PMID: 17728958 -
Abstract: PMID: 16648399 -
Abstract: PMID: 15902137 -
Abstract: PMID: 11945088 -
Abstract: PMID: 18178018 -
Abstract: PMID: 16698534 -
Abstract: PMID: 16435009 -
Abstract: PMID: 16989828 -
Abstract: PMID: 15735159 -
Abstract: PMID: 16091311 -
Abstract: PMID: 16026917 -
Abstract: PMID: 16738145 -
Abstract: PMID: 15191444 -
Abstract: PMID: 15191444 -
Abstract: PMID: 16563394 -
Abstract: PMID: 17845316 -
Abstract: PMID: 15118654 -
Abstract: PMID: 16946217 -
Abstract: PMID: 17222719 -
Abstract: PMID: 15339765 -
Abstract: PMID: 11672621 -
Abstract: PMID: 16026395 -
Abstract: PMID: 19755601 -
Abstract: PMID: 16310040 -
Abstract: PMID: 16458662 -
Abstract: PMID: 16959315 -
Abstract: PMID: 23887942 -
Abstract: PMID: 23887942 -
Abstract: PMID: 25425372 -
Abstract: PMID: 18310378 -
Abstract: PMID: 17139172 -
Abstract: PMID: 17365458 -
Abstract: PMID: 15167863 -
Abstract: PMID: 19306969 -
Abstract: PMID: 17689631 -
Abstract: PMID: 25402727 -
Abstract: PMID: 26338237 -
Abstract: PMID: 26444128 -
Abstract: PMID: 17634154 -
Abstract: PMID: 17573204 -
Abstract: PMID: 16965851 -
Abstract: PMID: 17097571 -
Abstract: PMID: 17904978 -
Abstract: PMID: 16502171 -
Abstract: PMID: 17980178 -
Abstract: PMID: 12523606 -
Abstract: PMID: 15971281 -
Abstract: PMID: 7788495 -
Abstract: PMID: 15118654 -
Abstract: PMID: 16858740 -
Abstract: PMID: 17327106 -
Abstract: PMID: 17688608 -
Abstract: PMID: 11243289 -
Abstract: PMID: 19021090 -
Abstract: PMID: 16582111 -
Abstract: PMID: 17355267 -
Abstract: PMID: 17514600 -
Abstract: PMID: 11339931 -
Abstract: PMID: 15863531 -
Abstract: PMID: 16582134 -
Abstract: PMID: 16728419 -
Abstract: PMID: 12548229 -
Abstract: PMID: 15369930 -
Abstract: PMID: 15134208 -
Abstract: PMID: 15914681 Calleja-Agius J, Custo R, Brincat MP, Calleja N. Placental abruption and placenta praevia. European Clinics in Obstetrics and Gynaecology. 2006 Nov;2(3):121-7. -
Abstract: PMID: 18439554 -
Abstract: PMID: 11798453 -
Abstract: PMID: 12297716 -
Abstract: PMID: 14655091 -
Abstract: PMID: 16563394
66