 Search
Search
Normal CNS Anatomy
Normal CNS Video
Above. Normal fetal CNS at 22 2/7ths weeks. Video courtesy of Dr. Mayank Chowdhury; Pallav Imaging Institute, Mayflower Women’s Hospital, Ahmedabad, India.
Above. Key fetal anatomy includes the choroid plexus, the septum cavum pellucidi (SCP), the lateral ventricles, and the corpus callosum. The pericallosal artery is a continuation of the anterior cerebral artery and it continues superiorly and posteriorly supplying the corpus callosum and the medial aspect of the cerebral hemisphere.
Key Views
There are three major scan planes for the fetal brain which accommodate 3 views:
1. Thalamic view
2. Ventricular view
3. Cerebellar view
The thalamic view is taken at the level of the biparietal diameter (BPD) and head circumference (HC).
The ventricular view is obtained through the atrium of the lateral ventricle.
The cerebellar view is angled through the posterior fossa (cisterna magna). All are axial (transverse) views of the fetal head with the exception of the cerebellar view, which is axial oblique. Other planes include the sagittal, parasagittal, and coronal which may be useful or necessary to define anatomy.
Thalamic View


Above. Thalamic view at 20 weeks. Note the thalamus and the position of the ambient cistern. The fornices are noted which are distinguished from the cavum septi pellucidi (CSP) by 3 parallel lines instead of the box like structure of the CSP.


Above. Thalamic view at 33 weeks gestation. Note the 3rd ventricle and again the fornices.

Above. This is the same acquisition plane for the BPD and HC. Visualization of the thalami, the midline falx, and the box-like cavum septi pellucidi (CSP) are possible. The presence or absence of the CSP is key to defining abnormal brain anatomy.
Ventricular View



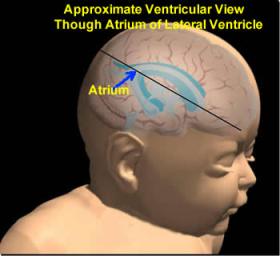
Above. This is a schematic of the lateral ventricles demonstrating the frontal, occipital, and temporal horns with the atrium of the lateral ventricle at the confluence of the occipital horn. The axial plane will demonstrate the lateral ventricles and the choroid plexus.


Above. This is an axial view demonstrating the atria of the lateral ventricle and the choroid plexus. The measurement is within normal limits.
Cerebellar View




Above. The cerebellar view is axial oblique with rotation of the transducer from the thalamic view to the cerebellum, while obtaining a view of the central cerebellar echogenic vermis. This view allows visualization of the cerebellum and cisterna magna (posterior fossa).
Cerebellar Measurements


Above. The cisterna magna or posterior fossa measurement is taken as illustrated from the outer aspect of the cerebellar vermis to the internal side of the occipital bone, and is normally between 2 mm and 10 mm in depth. The transcerebellar diameter is also measured as illustrated from outer to outer aspect of the cerebellum and varies by gestational age. Note the box like cavum septi pellucidi (CSP) which can also be seen with the cerebellar view.
Sagittal View
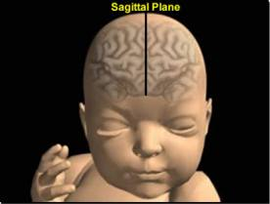

Above. The approximate sagittal plane which will demonstrate the corpus callosum, cavum septi pellucidi, and cavum vergae as well as the nasal bone.
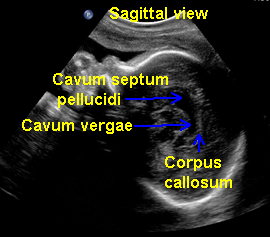

Above. The sagittal midline view of the brain. Note the corpus callosum, cavum septi pellucidi, and cavum vergae.
Parasagittal View
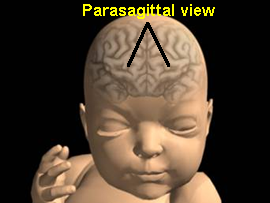
Above. Approximate parasagittal view. The parasagittal view allows visualization of the atrium, body, and anterior horn of the lateral ventricle and of the choroid plexus. It is not a commonly used view, but may be helpful in visualizing the atrium and the choroid plexus when the fetus is in breech presentation and the axial view is difficult to obtain.


Coronal View


Above. The approximate coronal views which can demonstrate the lateral ventricles, especially the frontal horns in an effort to determine whether there is fusion across the midline. The midbrain, choroid plexus, and cerebellum can also be assessed in this plane.




Above. This coronal view demonstrates the body of lateral ventricles and the midbrain. The coronal view may also demonstrate the echogenic choroid plexus. This view may be more easily obtained when the fetus is in breech presentation.
The transverse axial view permits visualization and measurement of the lateral ventricles as well as critical head measurements. It affords a view of the contents within the ventricle (blood or tumors) as well as an assessment of intracranial calcifications. The midsagittal view of the fetal brain best accomplishes visualization of the corpus callosum, cavum septum pellucidum, and posterior fossa.

Above. In breech presentation and transverse lie of the fetus, the midsagittal view can be obtained with a transabdominal scanning plane. With cephalic presentation, a transvaginal approach gives the best opportunity for midsagittal visualization. [1] The visualization of the septum pellucidum in all instances is helpful. Coronal views are useful for defining the site of ventricular communication and confirming the absence of the corpus callosum.

Above. Prenatal ultrasound evaluation of the fetal brain requires observation of specific structures, which in turn verify normality of other CNS structures. [2]

Above. The cavum septum pellucidum (CSP) and the cisterna magna (CM) are visible on trans-abdominal ultrasound between 16 weeks and 38 weeks. [2] Specific measurements of the CSP and CM differ significantly between the second and third trimester and correlate with biparietal diameter and gestational age. [3]

Above. The cavum septi pellucidi is critical to the diagnosis of a number of CNS malformations. [4] The presence of the CSP excludes complete agenesis of the corpus callosum while the absence of the CSP suggests the possibility of a number of other intracranial abnormalities, including septo-optic dysplasia.

Above. Septo-optic dysplasia is associated with a number of intracranial abnormalities. [5]

To define associated CNS malformations, other imaging modalities or views are necessary in addition to those obtained by routine trans-abdominal axial scan. These methods include transvaginal 2-D ultrasound and 3-D ultrasound. Above. 2-D transabdominal and transvaginal ultrasound may be the initial imaging modality of choice for schizencephaly, followed by 3-D ultrasound and fetal MRI. [6]
References
-
Abstract: PMID: 16238537 -
Abstract: PMID: 16344747 -
Abstract: PMID: 12692827 -
Abstract: PMID: 20194938 Septo-optic dysplasia. Erin E, Leonhardt BS, Tan-Sinn P. Journal of Diagnostic Medical Sonography. 2005; 21(6): 479-486. -
Abstract: PMID: 19536862
5