 Search
Search
Ebstein Anomaly: Imaging Considerations
Page Links: Ebstein’s Anomaly, Cardiomegaly, Cardiac Axis and Ebstein’s Anomaly, Distance between Tricuspid and Mitral Valve, High Pulsatility Index Ductus Venosus (DV), Supraventricular Tachycardia, Reveral of Flow; Ductus Arteriosus and Atrial Septum, Other Ultrasound Approaches in Ebstein’s, References
Definition

Ebstein anomaly accounts for about 0.5% of congenital heart defects. Ebstein anomaly is characterized by greater than 8 mm/m2 displacement of the septal and posterior tricuspid leaflets, which causes inflow tract “atrialization,” enlargement of the right atrium, and decrease in the size of the functional right ventricle. [1] The anterior leaflet of the tricuspid valve is redundant and large, but is not usually displaced. Color flow Doppler will show tricuspid regurgitation. One of the initial findings early in pregnancy is right atrial enlargement.

The following should be obtained if possible:

Right atrial size
On four chamber view, measure the distance (mm) between tricuspid and mitral valves (See nomogram: [2]).
Measure (mm) the mitral annulus (MA) and tricuspid annulus (TA).
Assess for tricuspid regurgitation with color Doppler flow.
Assess gradient across valves with pulsed Doppler.
Assess for pulmonary artery hypoplasia.
Assess for pericardial effusion.
Assess for cardiomegaly.
Assess the cardiac axis.
Assess the distance between mitral and tricuspid valve.
Cardiomegaly

Ebstein anomaly and tricuspid valve dysplasia are commonly associated with cardiac enlargement. Taken with a four chamber view in diastole, the cardiothoracic ratio is the circumference of the fetal heart in millimeters divided by the thoracic circumference in millimeters. [3] In Ebstein anomaly, the cardiothoracic ratio is commonly above .55.
In addition to Ebstein anomaly, the cardiothoracic ratio is increased in tricuspid dysplasia, atrioventricular septal defect, and complete heart block. [4] The cardiothoracic ratio is the circumference of the heart in mm divided by the circumference of the chest. (Normal values are from 0.45 at 17 weeks to 0.50 at term.)
Cardiac Axis and Ebstein Anomaly

The upper limit of normal of the fetal cardiac act axis is 44%. When the cardiac axis is greater than 57°, the likelihood of congenital heart defect is increased for Ebstein anomaly, pulmonary stenosis, coarctation of the aorta, and tetralogy of Fallot.


Above. Determination of cardiac axis. The 4-chamber view is obtained through a true transverse view of the fetal chest. The right ventricle is closest to the anterior chest wall and the left atrium is closest to the fetal spine. The fetal cardiac apex points to the left chest (levocardia). In a line perpendicular from the midline, the normal cardiac axis is 45 degrees (± 16 degrees).
Distance between Tricuspid and Mitral Valve
Ebstein anomaly causes a change in the appearance of the atrio-ventricular septum (AVS). In normal fetuses, the tricuspid valve is towards the apex of the heart compared to the mitral valve. The AVS is defined as the area between the insertion of the mitral valve and tricuspid leaflets to the ventricular septum. Nomogram’s are developed for the normal dimensions of the AVS, which can readily be compared to normal when Ebstein anomaly is suspected. [5]
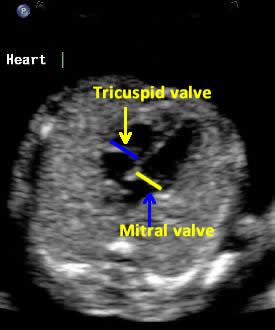

Above. Note the tricuspid valve is normally inferior and towards the apex of the heart compared to the mitral valve. In Ebstein anomaly, the septal and posterior leaflets are typically inferior to the normal tricuspid annulus.
High Pulsatility Index Ductus Venosus (DV)

High pulsatility index in the ductus venosus (DV) is commonly present in fetuses with right-sided cardiac lesions and obstruction to outflow. However, these changes do not indicate right-sided heart failure since they are likely due to the hemodynamic effect of lesions such as Ebstein anomaly. [6]
Supraventricular Tachycardia
Supraventricular tachycardia may be a presenting finding in patients with Ebstein anomaly. Early diagnosis is important since mortality is relatively high. [7]
Reversal of Flow, Ductus Arteriosus, and Atrial Septum
Doppler color flow mapping and pulsed or continuous wave Doppler can determine direction of blood flow across the ductus arteriosus or atrial septum. Reversal of shunting can be identified across either the ductus arteriosus or atrial septum. The prognosis is poor when there is reversal of flow in either of these shunts. [8]
Other Ultrasound Approaches in Ebstein Anomaly
Several applications of the STIC (spatio-temporal image correlation) technology has been successfully employed in the diagnosis of Ebstein anomaly. [9]
STIC acquisition in combination with inversion mode and virtual organ computer-aided analysis may be applicable to Ebstein anomaly since the process allows myocardial volume analysis. [10]
Three dimensional multiplanar ultrasound of Ebstein anomaly defines morphology and permits differentiation between Ebstein anomaly and tricuspid valve dysplasia. [11]