 Search
Search
Placenta Previa: Information
Page Links: Definition, Incidence, Risk Factors, Placental “Migration”, Symptoms, Outcome, Clinical Summary, References
Definition
Placenta previa is a placental implantation abnormality when any portion of the placenta covers or is near the internal cervical os.
Previous definitions include 3 groups:
• Complete placenta previa: the placenta covers the entire cervical os.
• Partial placenta previa: the edge of the placenta partially covers the internal cervical os.
• Marginal placenta previa: the placenta is at the margin of the internal cervical os but does not cover it.
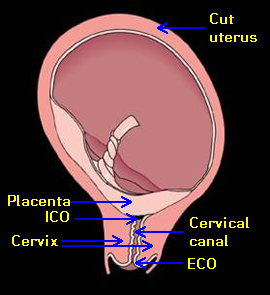

Above. This cut diagram of the uterus with complete placenta previa demonstrates the critical relationships between internal cervical os (ICO), the cervix, and the placenta. The cervical canal is illustrated as well as the external cervical os (ECO).


Above. Note the placenta partially covers the internal cervical os and is within 2 cm of the internal cervical os (ICO), but does not completely cover the os.
Transvaginal ultrasound permits accurate measurement of the distance between the internal cervical os and placental edge, and definitions are evolving:
Complete placenta previa: the placenta covers the internal cervical os.
Incomplete placenta previa: the leading edge of the placenta is within 2 cm of the internal os.
Low-lying placenta: the placenta is greater than 2 cm from the internal cervical os, but is in the lower 1/3 of the uterus.
Incidence

While the incidence varies by parity [1], the overall incidence is about 4.4 per 1000 births. [2]

Some reports suggest that the incidence is dependent upon a history of prior C-section [3], but prediction models for women with a history of 1 prior C-section show a low sensitivity (13%). [4] In addition, the odds ratio of 1.4 (95% CI 1.1,1.6) shows only a moderate risk for placental abruption and placenta previa as a long-term effect of previous C-section [5], while others show no predictive value of previous C-section for detecting placenta previa based upon a second trimester ultrasound scan. [6]
Risk Factors

Risk factors for placenta previa are subdivided into historical and present pregnancy categories. [7]
• Risk of placenta previa is nearly 3 times higher in pregnancies following assisted reproduction. [8]
• Rate of placenta previa is 40% higher among twins than singletons. [9]
Placental “Migration”

The apparent leading edge of the placenta may “migrate” from the lower uterine segment away from the region of the internal cervical os.
• Longitudinal ultrasound studies [10] demonstrate that the incidence of low-lying placenta is about 15% at 12 to 14 weeks gestation. However, 85% of these early abnormal placental implantation sites revert to normal by term.
• At 30 weeks gestation: 60% of partial placenta previas persist to term.
• At 30 weeks gestation: 75% of total placenta previas persist to term.
However, there is a greater persistence to term if there is a complete placenta previa or posterior placenta previa within 1 cm of the internal cervical os (ICO) [11], and a final placental distance of < 2.0 cm is associated with C-section and peripartum complications. [12]
Symptoms
The classic symptom of placenta previa is painless vaginal bleeding.
• Overall, the incidence of genital bleeding at > 24 weeks gestation is 2% to 5%. [13]
• Outcome is generally better for women with a history of light vaginal bleeding occurring between 16 and 24 weeks compared to women with heavy bleeding, while prognosis is worse in placenta previa patients with heavy bleeding. [14]
• Placenta previa patients have higher rates of [15]:
Second trimester bleeding (OR* 156.0, 95% CI** 87.2-277.5)
Abruptio placenta (OR 13.1, 95% CI 8.2-20.7)
Placenta accreta (OR 3.6, 95% CI 1.1-9.9)
Postpartum hemorrhage (OR 3.8, 95% CI 1.2-10.5)
Postpartum anemia (OR 5.5, 95% CI 4.4-6.9)
*OR=odds ratio; ** CI=confidence interval
Outcome

Increased use of transvaginal ultrasound increases diagnostic precision and links findings to potential clinical outcomes.
Sonographic features predictive of massive bleeding include [16]:
• Echo-free space in the lower edge of the placenta overlying cervix.
• Placental “lacunae.”
• Sponge-like echoes in adjacent uterine wall.
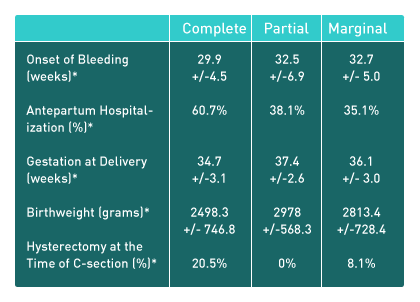
All outcomes: partial placenta previa did not differ from marginal placenta previa.
Women with complete placenta previa had significantly poorer outcomes compared to the other 2 groups.
Others show that pregnancy outcomes vary with the type and designation of placenta previa. [17]
The risks for complete placenta previa are greater than those of incomplete placenta previa and include an increased risk for the following [18]:
• Antepartum and postpartum transfusions
• Postpartum hemorrhage
• Postpartum hysterectomy
• Placenta accreta
• Low birth weight
Low-lying placenta:
Postpartum hemorrhage is the main adverse outcome for patients with low-lying placenta detected during the second trimester of pregnancy.
Clinical Summary
Placenta Previa Summary (based upon the above literature review).
Placenta previa definitions:
Complete placenta previa: the placenta covers all of the internal cervical os.
Incomplete placenta previa: the placenta is within 2 cm of the internal cervical os.
These changes in definition are due to the following factors:
• The accuracy of transvaginal ultrasound in defining the relationship between the leading placental edge and the internal cervical os.
• The poorer outcomes reported for complete placenta previa compared to partial and marginal placenta previa.
• The apparent non-difference in outcomes between partial and marginal placenta previa.
The incidence of placenta previa is from 1.9 to 3.9 per 1000 live births and is dependent upon parity and possibly upon a history of prior C-section.
Risk factors for placenta previa are:
• Historical: Prior C-section, pregnancy termination, increased parity, maternal age.
• Present pregnancy: Assisted reproduction, smoking, multi-fetal gestation.
• Symptoms/Associations: The primary symptom is genital bleeding, which occurs in 2% to 5 % of pregnancies of > 24 weeks and outcome is based upon the severity of bleeding.
Patients with placenta previa have higher rates of:
• Second-trimester bleeding
• Abruptio placenta
• Placenta accreta
• Postpartum hemorrhage
• Postpartum anemia
Placental “migration”:
• The findings on early ultrasound persist to term in only a small number of patients with a low-lying placenta or placenta previa.
• At 28 weeks and beyond, continued placental migration persists into the third trimester in some patients.
• At 28 to 32 weeks, complete placenta previa or posterior placenta previa within 1 cm of the internal cervical os (ICO) tends to persist.
Outcomes:
Ultrasound findings predictive of massive bleeding include:
• Echo-free space in the lower edge of the placenta overlying the cervix.
• Placental “lacunae.”
These findings are also associated with placenta accreta and explain their overlying relationship and significance for bleeding.
References
-
Abstract: PMID: 19021090 -
Abstract: PMID: 16582111 -
Abstract: PMID: 17355267 -
Abstract: PMID: 17514600 -
Abstract: PMID: 11339931 -
Abstract: PMID: 15863531 -
Abstract: PMID: 16582134 -
Abstract: PMID: 16728419 -
Abstract: PMID: 12548229 -
Abstract: PMID: 15369930 -
Abstract: PMID: 15134208 -
Abstract: PMID: 15914681 Calleja-Agius J, Custo R, Brincat MP, Calleja N. Placental abruption and placenta praevia. European Clinics in Obstetrics and Gynaecology. 2006 Nov;2(3):121-7. -
Abstract: PMID: 18439554 -
Abstract: PMID: 11798453 -
Abstract: PMID: 12297716 -
Abstract: PMID: 14655091 -
Abstract: PMID: 16563394
13