 Search
Search
Tetralogy of Fallot (TOF): Imaging Considerations
Page Links: Definition, Four Chamber View, 3 Vessel View, Fetal Cardiac Axis, 3-D and 4-D Ultrasound, STIC, Tomographic Ultrasound Imaging, References
Definition
Most conotrunchal fetal cardiac anomalies including Tetralogy of Fallot (TOF) can be diagnosed prenatally by fetal echocardiography, and among conotrunchal anomalies, TOF has the highest rate of prenatal detection (91.7%). [1] A fetus diagnosed with Tetralogy of Fallot may need surgery or other procedures soon after birth.

Tetralogy of Fallot is defined by four classic elements: misalignment of the VSD (ventricular septal defect), right displacement of the aorta (overriding aorta), hypertrophy of the right ventricle, and pulmonary stenosis (PS). Right ventricular hypertrophy does not usually occur until after birth, and pulmonary stenosis may not be present during early ultrasound examinations, but can develop or worsen during the latter part of the pregnancy. [2] During the second trimester, the VSD and overriding aorta is usually detected on four chamber cardiac views, but evaluation of the outflow tracts increases TOF’s detection rate.
Four Chamber View
Using a four chamber view and outflow tract analysis, the sensitivity for detecting congenital heart defects is approximately 89%, while conotruncal abnormalities can be suspected with the four chamber view. [3]
3 Vessel View
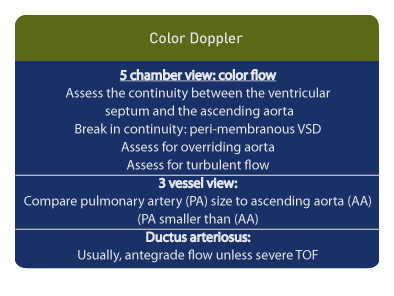
The fetal three vessel view (3VV) is useful for the diagnosis of Tetralogy of Fallot, and allows assessment of the superior vena cava, ascending aorta (AA), and main pulmonary artery (MPA) in that order.
“Classic” Tetralogy of Fallot is associated with pulmonary stenosis, while Tetralogy of Fallot with pulmonary atresia or absent pulmonary valve syndrome is considered a variant.

An enlarged and dilated aorta may present as the “question mark” sign in the three vessel view. When this finding is present, 69% of the fetuses had TOF with pulmonary stenosis, 21% had TOF with pulmonary atresia, and 9.5% had TOF with absent pulmonary valve syndrome. [4]

An aorta which is larger than the main pulmonary artery is associated with Tetralogy of Fallot. When the ratio of AA/MPA is greater than 1 in the three vessel view, 81% of the fetuses had TOF or a TOF variant, and 19% had an aortic valve abnormality. [5]
Fetal Cardiac Axis

The fetal cardiac axis is determined using the four chamber heart view and measuring the angle between the interventricular septum and a line bisecting the chest. The normal fetal cardiac axis is 43 + or – 7°. An abnormal cardiac axis of greater than 57° is associated with congenital heart defects, including Tetralogy of Fallot. [6]
3-D and 4-D Ultrasound
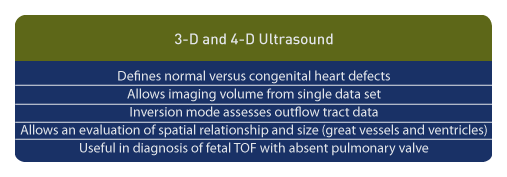
Real-time 3-D echocardiography has been employed to define normal versus congenital heart defects. This methodology allows imaging volume from a single data set; localization of tumors; and estimation of ventricular size and function are possible. [7] 4D ultrasound in the inversion mode evaluates the outflow tracts in 3-D real-time and allows an evaluation of the spatial relationship and size between the great vessels and between the ventricles. [8] Three and four-dimensional ultrasound is reported in the diagnosis of Tetralogy of Fallot with absent pulmonary valve. [9]
STIC

The STIC (spatio-temporal image correlation) technology allows measurement of the defect, its spatial location in relationship to the septum, and the time location in the cardiac cycle. [10] Data set volumes from STIC technology are manipulated in various ways. A novel method is to image the outflow tracts and ventricular septum by drawing dissecting lines through the four chamber view of the heart. This simple targeted arterial rendering (START) method may simplify analysis of fetal heart data. [11]
Tomographic Ultrasound Imaging (TUI)

Finally, tomographic ultrasound imaging (TUI) allows the sonographer to obtain data volume sets, which include the 4-chamber view, the 5-chamber view, the 3 vessel view, and tracheal views facilitating assessment of normal and abnormal cardiac anatomy. [12]
References
-
Abstract: PMID: 19481856 -
Abstract: PMID: 18726943 -
Abstract: PMID: 9087493 -
Abstract: PMID: 20205151 -
Abstract: PMID: 19106350 -
Abstract: PMID: 7800334 -
Abstract: PMID: 15906427 -
Abstract: PMID: 20598030 -
Abstract: PMID: 20552182 -
Abstract: PMID: 15690557 -
Abstract: PMID: 20878672 -
Abstract: PMID: 16301725